
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 37; 2025 > Article
- Original Article Health effects of weekend work on Korean workers: based on the 6th Korean Working Conditions Survey
-
Ji-Hyeon Lee1
 , Jin-Young Min2, Seok-Yoon Son1, Seung-Woo Ryoo1, Kyoung-Bok Min1,3,4,*
, Jin-Young Min2, Seok-Yoon Son1, Seung-Woo Ryoo1, Kyoung-Bok Min1,3,4,* -
Annals of Occupational and Environmental Medicine 2025;37:e31.
DOI: https://doi.org/10.35371/aoem.2025.37.e31
Published online: September 3, 2025
1Department of Preventive Medicine, Seoul National University College of Medicine, Seoul, Korea
2Veterans Medical Research Institute, Veterans Health Service Medical Center, Seoul, Korea
3Integrated Major in Innovative Medical Science, Seoul National University Graduate School, Seoul, Korea
4Institute of Environmental Medicine, Seoul National University Medical Research Center, Seoul, Korea
- *Corresponding author: Kyoung-Bok Min Department of Preventive Medicine, Seoul National University College of Medicine, 103 Daehak-ro, Jongno-gu, Seoul 03080, Korea E-mail: minkb@snu.ac.kr
• Received: June 25, 2025 • Revised: August 19, 2025 • Accepted: August 26, 2025
© 2025 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,353 Views
- 116 Download
Abstract
-
Background Although weekend work makes up a significant part of work patterns in modern society, research on the health effects of weekend work is relatively limited compared to other types of nonstandard work. This study was conducted to examine the impact of weekend work on the health of Korean workers, aiming to provide evidence to support the development of welfare policies that promote workers’ health.
-
Methods This study was conducted using data from the 6th Korean Working Conditions Survey, targeting 35,957 Korean workers who met the research criteria. Based on the survey responses, information was collected on weekend work status and health outcomes, including general health, musculoskeletal pain, headaches or eye pain, fatigue, sleep disorders, depression, anxiety, absenteeism and presenteeism. To examine the association between weekend work and health outcome variables, logistic regression analysis was performed adjusting for sociodemographic and occupational characteristics, with additional stratified analyses conducted according to employment status.
-
Results Among the final study population, 11,255 workers, accounting for 30.5% of the total, were weekend workers. After adjusting for sociodemographic and occupational characteristics, weekend work was found to be significantly associated with depression (odds ratio [OR]: 1.08; 95% confidence interval [CI]: 1.00–1.18), anxiety (OR: 1.35; 95% CI: 1.16–1.58), musculoskeletal pain (OR: 1.45; 95% CI: 1.34–1.58), fatigue (OR: 1.49; 95% CI: 1.36–1.62), absenteeism (OR: 1.70; 95% CI: 1.43–2.03), and presenteeism (OR: 1.82; 95% CI: 1.62–2.04). The health effects of weekend work differed between the self-employed and employees, as shown in the results of the stratified analysis.
-
Conclusions Weekend work was found to increase the risk of both physical and mental health problems of Korean workers, and the effect varied according to employment status. There is a need to design a comprehensive occupational health policy that reflects the characteristics of different employment statuses.
BACKGROUND
Labor regulations in many countries have been restructured to strengthen workers’ rights, including the implementation of statutory limits on weekly working hours. As a result, the 5-day workweek has become the normative standard across most industrialized economies. Nevertheless, nonstandard work schedules—particularly weekend work—remain a persistent and substantial feature of contemporary labor markets. In the United States, approximately 29% of employees reported working on weekends in 2022.1 In Europe, the prevalence averaged 25% in 2023, with notable cross-national variation.2 In Australia, nearly 30% of the workforce engaged in weekend work during the same period.3 In South Korea, the prevalence is even higher; as of 2020, 42.9% of workers reported working on Saturdays and 20.3% on Sundays,4,5 underscoring the widespread nature of weekend labor even under formal labor protections.
Weekend work is increasingly recognized as a socially embedded labor pattern, particularly in service-oriented, retail, and self-employment sectors that demand temporal flexibility.6 As labor markets shift toward deregulation and flexible scheduling, a growing number of workers are routinely assigned to or voluntarily engage in weekend shifts.7 However, this nonstandard schedule challenges conventional temporal boundaries between work and personal life, and is associated with a range of psychosocial and behavioral disruptions, including work-life conflict, reduced recovery time, and social disconnection.8,9
Emerging empirical evidence supports these concerns, indicating that weekend work may adversely affect workers’ health through both physiological and psychological pathways. Jamal (2004)10 found that employees working weekends experienced significantly higher levels of emotional exhaustion, job stress, and psychosomatic symptoms compared to their weekday-only counterparts. Similarly, Davis et al. (2008)11 observed elevated job strain among office workers engaged in weekend shifts. A population-based study in Japan further demonstrated that weekend work was strongly associated with poor mental health outcomes, with each additional hour of weekend labor exerting disproportionately greater psychological impact than equivalent weekday hours.12
Despite these findings, epidemiological evidence on the direct health consequences of weekend work remains limited and inconclusive. Moreover, little attention has been paid to how these health risks may differ by employment type—a potentially critical determinant of occupational vulnerability. Employment status fundamentally influences the degree of autonomy over work schedules, exposure to job-related stressors, and access to social protection.13 Self-employed workers may enjoy greater temporal flexibility but often face heightened economic insecurity and longer working hours.14,15 In contrast, employees are typically subject to fixed schedules and limited control, which may also contribute to work-related stress.16 These structural differences suggest that the health implications of weekend work are unlikely to be uniform across employment categories, highlighting the importance of disaggregated analysis.
In the South Korean context, where weekend work remains prevalent yet underexamined, there is a pressing need to clarify the health implications of this nonstandard work arrangement. The present study addresses this gap by investigating the associations between weekend work and multiple dimensions of health—including general, psychological, and physical health—using a nationally representative dataset. In addition, we examine whether these associations differ by employment status (self-employment vs. wage employment), thereby contributing novel insights into occupational health inequities in the context of nonstandard labor.
METHODS
This study was designed as a population-based, cross-sectional analysis, utilizing data from the 6th Korean Working Conditions Survey (KWCS). First launched in 2006, the KWCS is a nationwide survey targeting workers aged 15 and older who are engaged in economic activity in South Korea. The primary objective of the survey is to assess a broad range of employment and working conditions that may affect occupational safety and health. The 6th KWCS was conducted between October 5, 2020, and April 11, 2021.
Fig. 1 shows the sample selection process of our study. Of the 50,538 individuals originally surveyed, 1,605 unpaid family workers were excluded from the analysis. To isolate the effect of weekend work, an additional 12,290 individuals were excluded due to engagement in other forms of nonstandard work schedules—specifically, long working hours (defined as more than 52 hours per week), night work, or shift work—which may confound the health outcomes of interest. Furthermore, 686 respondents with missing data on key variables, such as weekend work status and health outcomes, were also excluded. After these exclusions, the final analytic sample comprised 35,957 participants. To assess data completeness, we calculated the response rate for each variable. To examine potential selection bias, we conducted chi-square tests to compare the characteristics of the included and excluded groups.
The main exposure variable in this study was weekend work status. This was defined based on participants’ responses to the question: “How many days per month do you work in the following categories?” If participants responded “None” to both “Saturday work” and “Sunday work”, they were classified as “non-weekend workers.” If they reported working one or more days on either day, they were categorized as "weekend workers."
Nine health-related variables were adopted as outcome variables. General health status was assessed using the question: “How would you describe your overall health?” Participants who answered “very poor” or “poor” were categorized as having “poor” general health, while those who answered “very good,” “good,” or “fair” were categorized as having “good” general health.
The risk of sleep disorders was assessed using the Minimal Insomnia Symptom Scale. Participants were asked: “In the past year, how often have you experienced the following sleep-related problems?” Each of the three sub-items (A, B, and C) was scored from 0 to 4, the total score was calculated. A total score of 6 or more indicated a “high” risk of insomnia.17 Depression was assessed using the World Health Organization Well-Being Index (WHO-5), based on responses to the question: “In the past two weeks, how often have you experienced the following feelings?” Each item was rated on a 6-point scale (1–6), and scores for five sub-items were summed. The total score was then multiplied by 4. A final score of 50 or less indicated a high risk of depression.18 Anxiety, and headaches or eye pain, and general fatigue were assessed with the question: “In the past year, have you experienced any of the following health issues?” Participants who answered “yes” were classified as having a “high” risk for each respective condition. Musculoskeletal pain was also measured using the same question. Participants were asked whether they had experienced pain in any of three regions: (A) back, (B) upper limbs, or (C) lower limbs. Those who reported at least one of these were classified as having a “high” risk of musculoskeletal pain.
To assess absenteeism due to health problems, participants were asked: “In the past year, how many days have you missed due to health-related issues?” Respondents who answered “1 day or more” were considered to have experienced absenteeism. Presenteeism, defined as attending work despite health problems, was assessed with the question: “In the past year, have you gone to workplace while feeling unhealthy?” Those who answered “yes” were categorized as having experienced presenteeism.
To control for potential confounders, sociodemographic and occupational characteristics were included as covariates. Sociodemographic variables included sex (male or female), age (15–29, 30–39, 40–49, 50–59, or ≥60 years), educational attainment (below college or college graduate), and monthly income level (<2,000,000 KRW; 2,000,000–2,999,999; 3,000,000–3,999,999; or ≥4,000,000 KRW). Occupational variables included employment status and weekly working hours. Employment status was classified into self-employed and employees. Weekly working hours were grouped into <40 hours and ≥40 hours, based on the Korean Labor Standards Act, which stipulates a 40-hour workweek as the legal maximum.
Descriptive analyses were conducted to examine the distribution of participants’ sociodemographic characteristics, occupational characteristics, and health outcomes according to weekend work status. Differences between weekend workers and non-weekend workers were assessed using chi-square tests for categorical variables.
To evaluate the association between weekend work and each health-related outcome, logistic regression analyses were performed. Two models were specified: a crude model, in which no covariate was adjusted, and an adjusted model, which controlled for sociodemographic characteristics (sex, age, educational attainment, and monthly income) and occupational factors (employment status and weekly working hours). For each outcome, odds ratios (ORs) and 95% confidence interval (CI) were estimated for weekend workers compared to non-weekend workers. Furthermore, to explore potential effect modification by employment status, stratified logistic regression analyses were conducted separately for self-employed individuals and employees. This approach enabled the assessment of whether the association between weekend work and health outcomes differed meaningfully between these two occupational groups. To assess the robustness of our findings, we conducted a sensitivity analysis by excluding workers who reported working 6 or 7 days per week. This allowed us to examine whether the observed health effects of weekend work persisted after reducing the potential confounding influence of total weekly workdays.
All analyses incorporated individual-level sampling weights provided by the 6th KWCS, which were calibrated using the March 2021 Economically Active Population Survey to ensure national representativeness. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and a two-tailed p-value < 0.05 was considered indicative of statistical significance.
Institutional Review Board (IRB) of Seoul National University Hospital determined to exempt the review of this study and approved the waiver of written informed consent due to the secondary use of anonymous information (IRB No. E-2208-111-1351).
RESULTS
Before presenting the main results, Supplementary Table 1 shows the variable-specific response rates for health variables with missing data due to non-response. A comparison of characteristics between the excluded group and the study population can be found in Supplementary Table 2. Chi-square test results showed significant differences between the study population and the excluded group in terms of sex, status of employment, and working hours, while no significant differences were found for the other variables.
Table 1 shows participants’ sociodemographic and occupational characteristics by weekend work status. Among the final analytic sample of 36,920 participants after applying the weights, 11,255 workers (30.5%) reported working on weekends. Overall, 55.8% of participants were male and 44.2% were female. Among weekend workers, the proportion of males was notably higher at 60.1%, compared to 39.9% for females. With respect to age, the 50–59 age group accounted for the largest share of weekend workers (24.9%), whereas the 15–29 age group represented the smallest proportion (15.2%). In terms of educational attainment, weekend workers were more likely to have an educational level below college (55.5%) compared to non-weekend workers (37.7%). For income, the most common category for both groups was less than 2 million KRW per month. Regarding occupational characteristics, weekend workers had a markedly higher proportion of self-employed individuals (31.3%) compared to non-weekend workers (10.4%). Additionally, a slightly higher proportion of weekend workers (26.7%) reported working less than 40 hours per week compared to non-weekend workers (24.5%). All sociodemographic and occupational variables differed significantly between weekend and non-weekend workers (p < 0.05).
Table 2 summarizes the distribution of health outcomes by weekend work status. Weekend workers exhibited significantly higher prevalence rates of poor general health, psychological distress (including depression and anxiety), absenteeism due to illness, and presenteeism compared to their non-weekend counterparts. For physical health conditions, the prevalence of musculoskeletal pain and fatigue was also significantly elevated among weekend workers.
Table 3 shows the results of logistic regression analyses assessing the association between weekend work and various health-related outcomes. In the crude model, weekend work showed significant associations with all health indicators examined in this study. After adjusting for sociodemographic and occupational covariates, weekend work remained significantly associated with depression (OR: 1.08; 95% CI: 1.00–1.18), anxiety (OR: 1.35; 95% CI: 1.16–1.58), musculoskeletal pain (OR: 1.45; 95% CI: 1.34–1.58), fatigue (OR: 1.49; 95% CI: 1.36–1.62), absenteeism due to illness (OR: 1.70; 95% CI: 1.43–2.03), and presenteeism (OR: 1.82; 95% CI: 1.62–2.04). No statistically significant associations were observed for general health, sleep disorder, headaches, or eye pain after covariate adjustment.
Table 4 shows the stratified analyses by employment status (self-employed vs. employees) to explore potential differences in the health impacts of weekend work. Among the self-employed, weekend work was significantly associated with musculoskeletal pain (OR: 1.47; 95% CI: 1.24–1.73), fatigue (OR: 1.37; 95% CI: 1.15–1.63), absenteeism (OR: 2.34; 95% CI: 1.58–3.46), and presenteeism (OR: 2.20; 95% CI: 1.71–2.84), but not with depression or anxiety. In contrast, among employees, weekend work was significantly associated with depression (OR: 1.11; 95% CI: 1.01–1.22), anxiety (OR: 1.40; 95% CI: 1.17–1.68), musculoskeletal pain (OR: 1.45; 95% CI: 1.32–1.59), fatigue (OR: 1.52; 95% CI: 1.38–1.67), absenteeism (OR: 1.59; 95% CI: 1.30–1.94), and presenteeism (OR: 1.75; 95% CI: 1.54–1.99). Notably, the odds for fatigue was higher among employees, whereas musculoskeletal pain, absenteeism, and presenteeism exhibited stronger associations among the self-employed. No significant associations were found for general health, sleep disorders, headaches, or eye pain in either employment group.
The results of the sensitivity analysis are presented in Supplementary Table 3. Similar to the primary analysis, weekend work remained significantly associated with depression, anxiety, musculoskeletal pain, fatigue, absenteeism, and presenteeism even after excluding workers who worked 6 or 7 days per week.
DISCUSSION
In this nationally representative cohort, nearly 30% of economically active individuals reported working on weekends-a strikingly high prevalence that reflects the evolving dynamics of modern labor markets. Weekend workers were socioeconomically disadvantaged, characterized by lower educational attainment, reduced income levels, and a substantially higher rate of self-employment. Beyond these structural disparities, weekend work was significantly associated with a broad spectrum of adverse health outcomes. After controlling for sociodemographic and occupational covariates, weekend workers exhibited elevated risk of fatigue, musculoskeletal pain, absenteeism, and presenteeism, as well as poorer mental health profiles, including higher OR of depression and anxiety. These findings suggest that weekend work may serve not merely as a marker of labor precarity, but as an independent determinant of physical and psychological morbidity. The results of the sensitivity analysis, excluding workers who worked 6 or 7 days per week, were largely consistent with those of the main analysis, demonstrating the robustness of our findings.
Our findings are broadly consistent with prior research conducted in Europe and other developed countries, which have consistently demonstrated the health risks associated with weekend work. For example, studies based on the European Working Conditions Survey19,20 have found that workers engaged in weekend shifts are more likely to experience occupational accidents—likely due to disrupted work-rest cycles, cumulative fatigue, and reduced staffing during weekends. Other studies have shown that weekend workers tend to engage in lower levels of physical activity and higher alcohol consumption, lifestyle factors that can further exacerbate physical health risks.21 Together, these patterns suggest that weekend work may contribute to a cumulative physiological burden, elevating the risk for both acute injuries and chronic conditions.
In addition to physical health concerns, the psychological burden of weekend work has been widely documented. Weston et al. (2019)22 identified a strong association between weekend work and depressive symptoms. A key mechanism appears to be the erosion of work-life balance, as highlighted in earlier work by Wirtz et al.19 and Greubel et al.,20 which limits opportunities for recovery and increases emotional strain. Moreover, weekend shifts often interfere with time spent with family and social networks, as shown in studies by Bittman (2005)23 and Lass and Wooden (2022),24 further contributing to stress, social isolation, and relational conflict—all of which are linked to poor mental health outcomes.25
Weekend work was also significantly associated with elevated levels of both absenteeism and presenteeism. These dual outcomes were particularly pronounced among self-employed workers, who may face competing pressures: a strong sense of financial and personal responsibility that drives them to work while ill, and greater flexibility that permits time off when necessary.26,27 By contrast, employees may be constrained by a lack of paid sick leave or workplace culture discouraging absence, resulting in suppressed absenteeism and potentially higher presenteeism. This interpretation aligns with cross-national evidence; in countries like Germany, where paid sick leave is guaranteed, wage workers report higher absenteeism, whereas in South Korea, the absence of such protections may lead to greater presenteeism.28
These observed disparities can be further understood through Karasek’s Job Demand–Control model.29,30 Self-employed workers often benefit from greater job control, allowing them to regulate their workload and schedules, which may buffer psychological strain.31,32 Employees, on the other hand, are typically subject to fixed hours and hierarchical oversight, reducing their autonomy and increasing stress exposure. Previous studies have shown that job-related stress is one of the risk factors closely associated with mental health disorders like depression33,34 and anxiety.35 Our findings reflect this contrast: employees reported greater mental health burdens, while self-employed individuals exhibited greater presenteeism and absenteeism.
These findings have important implications for occupational health policy. In South Korea—where 23.5% of the labor force is self-employed—current labor protections fall short.36 Self-employed workers remain largely outside the scope of key labor laws, including the Labor Standards Act and Industrial Accident Compensation Insurance.37 There is a critical need to expand the legal definition of "worker" to include the self-employed and to improve access to public health and social safety nets. For employees, introducing statutory paid sick leave is essential to reducing presenteeism and supporting recovery. South Korea is one of the few Organisation for Economic Co-operation and Development countries without such provisions.38
This study’s strengths include its use of data from the 6th KWCS, which includes a large sample of over 50,000 individuals, thereby ensuring high reliability. The sample was selected to provide balanced representation across regions, age groups, and occupations, minimizing selection bias. Furthermore, sampling weights were applied to reflect the population structure, enhancing the generalizability of the findings to the entire Korean workforce. In addition, this study enabled a focused assessment of weekend work by excluding night, shift, and long-hour work, and it is also the first Korean study to explore the health risks of weekend work by employment type. However, several limitations should be noted. First, since the analysis of certain health variables such as musculoskeletal pain, headaches, or eye pain relied on self-reported responses without standardized diagnostic instruments, which may have introduced recall bias or misclassification. Second, the KWCS lacks information on broader systemic health conditions (e.g., cardiovascular, respiratory, and digestive disorders), limiting the generalizability of our findings to overall physical health. Third, key behavioral and medical confounders-such as alcohol consumption, smoking, and chronic disease history-were not available in the dataset, which may have influenced the observed associations. Fourth, the study did not account for job category or industry, which could influence the likelihood of weekend work and health outcomes, thus introducing residual confounding. Fifth, although this study benefits from the use of a large-scale, nationally representative dataset, there are limitations in the generalizability of its findings. The data were collected during the coronavirus disease 2019 pandemic, a period marked by atypical working conditions that may have influenced the results. In addition, the exclusion of workers in other nonstandard employment arrangements limits the applicability of the findings to the entire workforce. Therefore, caution should be exercised when generalizing these results to the broader working population. Lastly, the cross-sectional design precludes causal inference, as it is not possible to establish temporal directionality between weekend work and adverse health effects.
CONCLUSIONS
Weekend work is significantly associated with a range of adverse health outcomes, with varying effects by employment status. These findings support the need for differentiated and inclusive occupational health policies, alongside future longitudinal research to better understand the mechanisms linking weekend work to worker health.
Abbreviations
-
Funding
This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and Technology (grant number, RS-2022-NR070347, RS-2024-00338688).
-
Competing interests
Kyoung-Bok Min, contributing editor of the Annals of Occupational and Environmental Medicine, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
-
Author contributions
Conceptualization: Lee JH, Min KB. Data curation: Lee JH, Ryoo SW. Formal analysis: Lee JH. Funding acquisition: Min KB. Methodology: Lee JH, Min KB. Software: Lee JH. Validation: Min JY, Min KB. Visualization: Lee JH, Son SY. Writing - original draft: Lee JH, Min JY. Writing - review & editing: Min KB, Ryoo SW, Son SY.
-
Acknowledgments
The authors thank the Occupational Safety and Health Research Institute of Korea.
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Table 1.
Response rates for each variable with missing values.
Supplementary Table 2.
Comparison of participants’ characteristics between the study population and the excluded group.
Supplementary Table 3.
ORs (95% CIs) for health outcomes of weekend workers to non-weekend workers, restricted to individuals working ≤5 days/week (sensitivity analysis).
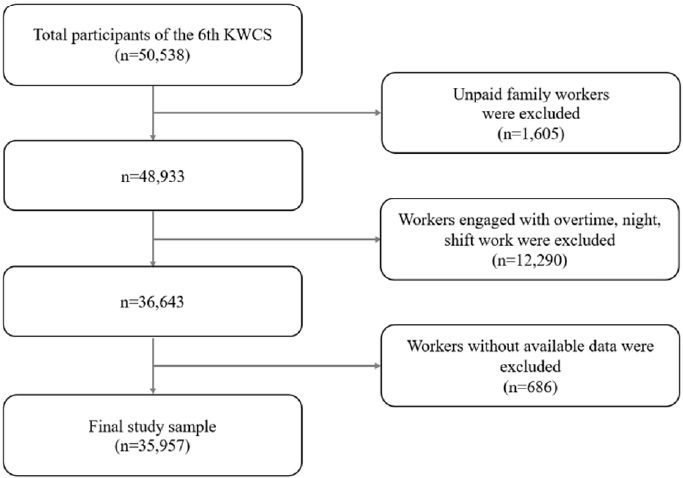
Table 1.
Participants’ characteristics according to weekend work status
| Characteristic | Total |
Weekend work |
p-value | |
|---|---|---|---|---|
| No | Yes | |||
| Total | 36,920 | 25,665 (69.5) | 11,255 (30.5) | |
| Sex | <0.001*** | |||
| Male | 20,597 (55.8) | 13,835 (53.9) | 6,763 (60.1) | |
| Female | 16,322 (44.2) | 11,830 (46.1) | 4,492 (39.9) | |
| Age (years) | <0.001*** | |||
| 15–29 | 5,110 (13.8) | 3,400 (13.3) | 1,711 (15.2) | |
| 30–39 | 7,439 (20.2) | 5,651 (22.0) | 1,788 (15.9) | |
| 40–49 | 8,914 (24.1) | 6,499 (25.3) | 2,415 (21.5) | |
| 50–59 | 8,379 (22.7) | 5,578 (21.7) | 2,800 (24.9) | |
| ≥60 | 7,078 (19.2) | 4,536 (17.7) | 2,541 (22.6) | |
| Education | <0.001*** | |||
| High-school graduate or lower | 15,909 (43.1) | 9,670 (37.7) | 6,240 (55.5) | |
| College graduate | 20,964 (56.8) | 15,959 (62.3) | 5,005 (44.5) | |
| Monthly income (10,000 KRW) | <0.001*** | |||
| <200 | 10,806 (29.3) | 7,258 (29.8) | 3,547 (32.9) | |
| 200–299 | 10,491 (28.4) | 7,092 (29.1) | 3,399 (31.5) | |
| 300–399 | 7,375 (20.0) | 5,193 (21.3) | 2,182 (20.2) | |
| ≥400 | 6,506 (17.6) | 4,841 (19.9) | 1,664 (15.4) | |
| Status of employment | <0.001*** | |||
| Self-employed | 6,188 (16.8) | 2,669 (10.4) | 3,520 (31.3) | |
| Employee | 30,731 (83.2) | 22,996 (89.6) | 7,735 (68.7) | |
| Work hours per week | 0.003** | |||
| <40 | 9,277 (25.1) | 6,274 (24.5) | 3,003 (26.7) | |
| 40–52 | 27,642 (74.9) | 19,391 (75.6) | 8,252 (73.3) | |
Table 2.
Prevalence of the health outcomes according to weekend work status
| Health outcomes |
Weekend work |
p-value | |
|---|---|---|---|
| No | Yes | ||
| General health | |||
| Poor | 929 (3.6) | 527 (4.7) | <0.001*** |
| Psychological health | |||
| Sleep disorder | 1,901 (7.4) | 967 (8.6) | 0.006** |
| Depression | 7,590 (29.6) | 3,734 (33.2) | <0.001*** |
| Anxiety | 1,105 (4.3) | 656 (5.8) | <0.001*** |
| Physical health | |||
| Musculoskeletal pain | 9,133 (35.6) | 5,272 (46.8) | <0.001*** |
| Headache or eye pain | 4,965 (19.4) | 1,979 (17.6) | 0.009** |
| Fatigue | 5,251 (20.5) | 3,196 (28.4) | <0.001*** |
| Sickness absence | |||
| Have experienced | 759 (3.0) | 551 (4.9) | <0.001*** |
| Presenteeism | |||
| Have experienced | 2,170 (8.5) | 1,585 (14.1) | <0.001*** |
Table 3.
ORs (95% CIs) for health outcomes of weekend workers to non-weekend workers
| Health outcomes |
Crude model |
Adjusted modela |
||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| General health | ||||
| Poor | 1.31 (1.13–1.52) | <0.001*** | 1.11 (0.95–1.29) | 0.210 |
| Psychological health | ||||
| Sleep disorder | 1.18 (1.05–1.32) | 0.006** | 1.11 (0.98–1.27) | 0.093 |
| Depression | 1.18 (1.10–1.27) | <0.001*** | 1.08 (1.00–1.18) | 0.049* |
| Anxiety | 1.38 (1.18–1.60) | <0.001*** | 1.35 (1.16–1.58) | <0.001*** |
| Physical health | ||||
| Musculoskeletal pain | 1.60 (1.49–1.71) | <0.001*** | 1.45 (1.34–1.58) | <0.001*** |
| Headache or eye pain | 0.89 (0.82–0.97) | 0.009** | 0.98 (0.89–1.07) | 0.607 |
| Fatigue | 1.54 (1.43–1.67) | <0.001*** | 1.49 (1.36–1.62) | <0.001*** |
| Sickness absence | ||||
| Have experienced | 1.69 (1.41–2.01) | <0.001*** | 1.70 (1.43–2.03) | <0.001*** |
| Presenteeism | ||||
| Have experienced | 1.77 (1.59–1.98) | <0.001*** | 1.82 (1.62–2.04) | <0.001*** |
Table 4.
ORs (95% CIs) for health outcomes of weekend workers to non-weekend workers, stratified by status of employment
| Health outcomes |
Crude model |
Adjusted modela |
||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| Self-employed | ||||
| General health | ||||
| Poor | 1.50 (1.19–1.90) | <0.001*** | 1.31 (1.00–1.72) | 0.053 |
| Psychological health | ||||
| Sleep disorder | 1.12 (0.90–1.38) | 0.307 | 1.03 (0.82–1.30) | 0.796 |
| Depression | 1.07 (0.92–1.25) | 0.362 | 0.98 (0.83–1.15) | 0.758 |
| Anxiety | 1.19 (0.90–1.58) | 0.214 | 1.17 (0.89–1.55) | 0.264 |
| Physical health | ||||
| Musculoskeletal pain | 1.70 (1.46–1.97) | <0.001*** | 1.47 (1.24–1.73) | <0.001*** |
| Headache or eye pain | 0.84 (0.70–1.03) | 0.087 | 0.86 (0.71–1.06) | 0.151 |
| Fatigue | 1.49 (1.25–1.78) | <0.001*** | 1.37 (1.15–1.63) | <0.001*** |
| Sickness absence | ||||
| Have experienced | 2.35 (1.63–3.38) | <0.001*** | 2.34 (1.58–3.46) | <0.001*** |
| Presenteeism | ||||
| Have experienced | 2.26 (1.77–2.89) | <0.001*** | 2.20 (1.71–2.84) | <0.001*** |
| Employee | ||||
| General health | ||||
| Poor | 0.89 (0.73–1.08) | 0.238 | 0.97 (0.79–1.20) | 0.779 |
| Psychological health | ||||
| Sleep disorder | 1.07 (0.93–1.24) | 0.350 | 1.13 (0.97–1.31) | 0.116 |
| Depression | 1.15 (1.05–1.26) | 0.002** | 1.11 (1.01–1.22) | 0.025* |
| Anxiety | 1.37 (1.14–1.64) | <0.001*** | 1.40 (1.17–1.68) | <0.001*** |
| Physical health | ||||
| Musculoskeletal pain | 1.40 (1.29–1.53) | <0.001*** | 1.45 (1.32–1.59) | <0.001*** |
| Headache or eye pain | 0.90 (0.81–1.00) | 0.051 | 1.00 (0.90–1.11) | 0.983 |
| Fatigue | 1.47 (1.34–1.62) | <0.001*** | 1.52 (1.38–1.67) | <0.001*** |
| Sickness absence | ||||
| Have experienced | 1.57 (1.28–1.91) | <0.001*** | 1.59 (1.30–1.94) | <0.001*** |
| Presenteeism | ||||
| Have experienced | 1.65 (1.46–1.87) | <0.001*** | 1.75 (1.54–1.99) | <0.001*** |
- 1. Bureau of Labor Statistics. American time use survey-2022 results, Table 4. Employed persons working and time spent working on days worked by full- and part-time status and sex, jobholding status, educational attainment, and day of week, 2023 annual averages. https://www.bls.gov/news.release/archives/atus_06222023.pdf. Updated 2023. Accessed May 28, 2025..
- 2. Eurostat. Work on weekends by sex, age, professional status and occupation. http://ec.europa.eu/eurostat/web/products-datasets/-/lfsa_qoe_3b3. Updated 2024. Accessed May 28, 2025..
- 3. Australian Bureau of Statistics. Characteristics of employment, Australia. https://www.abs.gov.au/statistics/labour/earnings-and-working-conditions/characteristics-employment-australia/latest-release. Updated 2024. Accessed May 28, 2025..
- 4. Korea Occupational Safety & Health Agency. Korean working conditions survey, 2020, work on saturdays. https://kosis.kr/statHtml/statHtml.do?orgId=380&tblId=DT_380002_D014_6TH&conn_path=I2. Updated 2022. Accessed May 28, 2025..
- 5. Korea Occupational Safety & Health Agency. Korean working conditions survey, 2020, work on sundays. https://kosis.kr/statHtml/statHtml.do?orgId=380&tblId=DT_380002_D013_6TH&conn_path=I2. Updated 2022. Accessed May 28, 2025..
- 6. Zeytinoglu IU, Cooke GB. Who is working at weekends? Determinants of regular weekend work in Canada. In: Boulin JV, Lallement M, Messenger J, Michon F, editors. Decent Working Time: New Trends, New Issues. Geneva, Switzerland: International Labour Organization; 2006, 395–416.
- 7. Berg P, Bosch G, Charest J. Working-time configurations: a framework for analyzing diversity across countries. ILR Rev 2014;67(3):805–37.
- 8. Anttila T, Oinas T. 24/7 Society: the new timing of work?. In: Tammelin M, editor. Family, Work and Well-Being: Emergence of New Issues. Cham, Germany: Springer International Publishing; 2018, 63–76.
- 9. Kalil A, Ziol-Guest KM, Levin Epstein J. Nonstandard work and marital instability: evidence from the national longitudinal survey of youth. J Marriage Fam 2010;72:1289–300.
- 10. Jamal M. Burnout, stress and health of employees on non‐standard work schedules: a study of Canadian workers. Stress Health 2004;20(3):113–9.Article
- 11. Davis KD, Goodman WB, Pirretti AE, Almeida DM. Nonstandard work schedules, perceived family well-being, and daily stressors. J Marriage Fam 2008;70(4):991–1003.ArticlePubMedPMC
- 12. Sato K, Kuroda S, Owan H. Mental health effects of long work hours, night and weekend work, and short rest periods. Soc Sci Med 2020;246:112774.ArticlePubMed
- 13. Nikolova M, Nikolaev B, Boudreaux C. Being your own boss and bossing others: the moderating effect of managing others on work meaning and autonomy for the self-employed and employees. Small Bus Econ 2023;60(2):463–83.ArticlePDF
- 14. Hyytinen A, Ruuskanen OP. Time use of the self‐employed. Kyklos 2007;60(1):105–22.Article
- 15. Parker SC, Belghitar Y, Barmby T. Wage uncertainty and the labour supply of self‐employed workers. Econ J 2005;115(502):C190–207.Article
- 16. Zhang N, He X. Role stress, job autonomy, and burnout: the mediating effect of job satisfaction among social workers in China. J Soc Serv Res 2022;48(3):365–75.Article
- 17. Westergren A, Broman JE, Hellstrom A, Fagerstrom C, Willman A, Hagell P. Measurement properties of the minimal insomnia symptom scale as an insomnia screening tool for adults and the elderly. Sleep Med 2015;16(3):379–84.ArticlePubMed
- 18. Topp CW, Ostergaard SD, Sondergaard S, Bech P. The WHO-5 Well-Being Index: a systematic review of the literature. Psychother Psychosom 2015;84(3):167–76.ArticlePubMedPDF
- 19. Wirtz A, Nachreiner F, Rolfes K. Working on Sundays-effects on safety, health, and work-life balance. Chronobiol Int 2011;28(4):361–70.ArticlePubMed
- 20. Greubel J, Arlinghaus A, Nachreiner F, Lombardi DA. Higher risks when working unusual times? A cross-validation of the effects on safety, health, and work-life balance. Int Arch Occup Environ Health 2016;89(8):1205–14.ArticlePubMedPDF
- 21. Thomas C, Power C. Shift work and risk factors for cardiovascular disease: a study at age 45 years in the 1958 British birth cohort. Eur J Epidemiol 2010;25(5):305–14.ArticlePubMedPDF
- 22. Weston G, Zilanawala A, Webb E, Carvalho LA, McMunn A. Long work hours, weekend working and depressive symptoms in men and women: findings from a UK population-based study. J Epidemiol Community Health 2019;73(5):465–74.ArticlePubMedPMC
- 23. Bittman M. Sunday working and family time. Lab Ind 2005;16(1):59–81.Article
- 24. Lass I, Wooden M. Weekend work and work-family conflict: evidence from Australian panel data. J Marriage Fam 2022;84(1):250–72.Article
- 25. Frone MR. Work-family conflict and employee psychiatric disorders: the National Comorbidity Survey. J Appl Psychol 2000;85(6):888–95.ArticlePubMed
- 26. Vinberg S, Landstad BJ, Tjulin A, Nordenmark M. Sickness presenteeism among the Swedish self-employed during the COVID-19 pandemic. Front Psychol 2021;12:723036.ArticlePubMedPMC
- 27. Hansen CD, Andersen JH. Going ill to work: what personal circumstances, attitudes and work-related factors are associated with sickness presenteeism? Soc Sci Med 2008;67(6):956–64.ArticlePubMed
- 28. Lechmann DS, Schnabel C. Absence from work of the self‐employed: a comparison with paid employees. Kyklos 2014;67(3):368–90.ArticlePDF
- 29. Karasek RA Jr. Job demands, job decision latitude, and mental strain: implications for job redesign. Admin Sci Q 1979;24:285–308.Article
- 30. Snyder LA, Krauss AD, Chen PY, Finlinson S, Huang YH. Occupational safety: application of the job demand-control-support model. Accid Anal Prev 2008;40(5):1713–23.ArticlePubMed
- 31. Hessels J, Rietveld CA, van der Zwan P. Self-employment and work-related stress: the mediating role of job control and job demand. J Bus Ventur 2017;32(2):178–96.Article
- 32. Stephan U, Roesler U. Health of entrepreneurs versus employees in a national representative sample. J Occup Org Psychol 2010;83(3):717–38.Article
- 33. Tennant C. Work-related stress and depressive disorders. J Psychosom Res 2001;51(5):697–704.ArticlePubMed
- 34. Wang J. Work stress as a risk factor for major depressive episode(s). Psychol Med 2005;35(6):865–71.ArticlePubMed
- 35. Godin I, Kittel F, Coppieters Y, Siegrist J. A prospective study of cumulative job stress in relation to mental health. BMC Public Health 2005;5:67.ArticlePubMedPMCPDF
- 36. Organisation for Economic Co-operation and Development. Self-employment rate. https://www.oecd.org/en/data/indicators/self-employment-rate.html. Updated 2023. Accessed May 28, 2025..
- 37. Park J, Han B, Kim Y. Comparison of occupational health problems of employees and self-employed individuals who work in different fields. Arch Environ Occup Health 2020;75(2):98–111.ArticlePubMed
- 38. Heymann J, Rho HJ, Schmitt J, Earle A. Ensuring a healthy and productive workforce: comparing the generosity of paid sick day and sick leave policies in 22 countries. Int J Health Serv 2010;40(1):1–22.ArticlePubMedPDF
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
Cite- Figure
-
- Related articles
-
- The relations among workplace verbal abuse, job stress, and good self-rated health among Korean wage workers: Evidence from the 7th Korean Working Conditions Survey (KWCS)
- Association between working ≥10 hours per day and satisfaction with work environment among wage workers in Korea: a cross-sectional study using data from the 7th Korean Working Conditions Survey
- Occupation classification model based on DistilKoBERT: using the 5th and 6th Korean Working Condition Surveys
- Association between single-person household wage workers in South Korea and insomnia symptoms: the 6th Korean Working Conditions Survey (KWCS)
Health effects of weekend work on Korean workers: based on the 6th Korean Working Conditions Survey
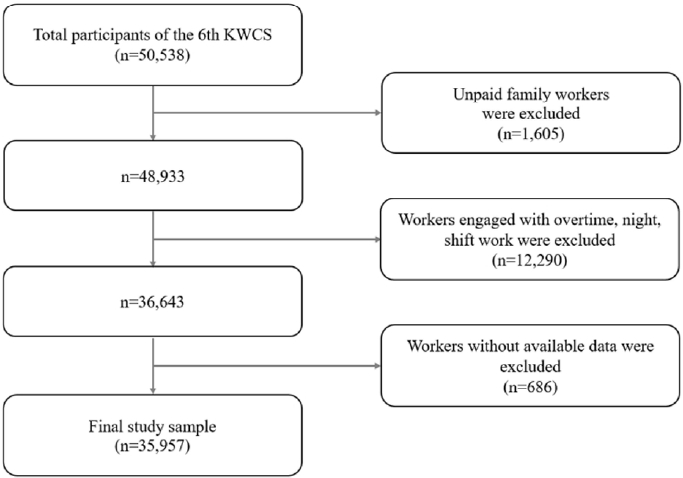
Fig. 1. Sample selection process with inclusion and exclusion criteria.
Fig. 1.
Health effects of weekend work on Korean workers: based on the 6th Korean Working Conditions Survey
| Characteristic | Total | Weekend work |
p-value | |
|---|---|---|---|---|
| No | Yes | |||
| Total | 36,920 | 25,665 (69.5) | 11,255 (30.5) | |
| Sex | <0.001 |
|||
| Male | 20,597 (55.8) | 13,835 (53.9) | 6,763 (60.1) | |
| Female | 16,322 (44.2) | 11,830 (46.1) | 4,492 (39.9) | |
| Age (years) | <0.001 |
|||
| 15–29 | 5,110 (13.8) | 3,400 (13.3) | 1,711 (15.2) | |
| 30–39 | 7,439 (20.2) | 5,651 (22.0) | 1,788 (15.9) | |
| 40–49 | 8,914 (24.1) | 6,499 (25.3) | 2,415 (21.5) | |
| 50–59 | 8,379 (22.7) | 5,578 (21.7) | 2,800 (24.9) | |
| ≥60 | 7,078 (19.2) | 4,536 (17.7) | 2,541 (22.6) | |
| Education | <0.001 |
|||
| High-school graduate or lower | 15,909 (43.1) | 9,670 (37.7) | 6,240 (55.5) | |
| College graduate | 20,964 (56.8) | 15,959 (62.3) | 5,005 (44.5) | |
| Monthly income (10,000 KRW) | <0.001 |
|||
| <200 | 10,806 (29.3) | 7,258 (29.8) | 3,547 (32.9) | |
| 200–299 | 10,491 (28.4) | 7,092 (29.1) | 3,399 (31.5) | |
| 300–399 | 7,375 (20.0) | 5,193 (21.3) | 2,182 (20.2) | |
| ≥400 | 6,506 (17.6) | 4,841 (19.9) | 1,664 (15.4) | |
| Status of employment | <0.001 |
|||
| Self-employed | 6,188 (16.8) | 2,669 (10.4) | 3,520 (31.3) | |
| Employee | 30,731 (83.2) | 22,996 (89.6) | 7,735 (68.7) | |
| Work hours per week | 0.003 |
|||
| <40 | 9,277 (25.1) | 6,274 (24.5) | 3,003 (26.7) | |
| 40–52 | 27,642 (74.9) | 19,391 (75.6) | 8,252 (73.3) | |
| Health outcomes | Weekend work |
p-value | |
|---|---|---|---|
| No | Yes | ||
| General health | |||
| Poor | 929 (3.6) | 527 (4.7) | <0.001 |
| Psychological health | |||
| Sleep disorder | 1,901 (7.4) | 967 (8.6) | 0.006 |
| Depression | 7,590 (29.6) | 3,734 (33.2) | <0.001 |
| Anxiety | 1,105 (4.3) | 656 (5.8) | <0.001 |
| Physical health | |||
| Musculoskeletal pain | 9,133 (35.6) | 5,272 (46.8) | <0.001 |
| Headache or eye pain | 4,965 (19.4) | 1,979 (17.6) | 0.009 |
| Fatigue | 5,251 (20.5) | 3,196 (28.4) | <0.001 |
| Sickness absence | |||
| Have experienced | 759 (3.0) | 551 (4.9) | <0.001 |
| Presenteeism | |||
| Have experienced | 2,170 (8.5) | 1,585 (14.1) | <0.001 |
| Health outcomes | Crude model |
Adjusted model |
||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| General health | ||||
| Poor | 1.31 (1.13–1.52) | <0.001 |
1.11 (0.95–1.29) | 0.210 |
| Psychological health | ||||
| Sleep disorder | 1.18 (1.05–1.32) | 0.006 |
1.11 (0.98–1.27) | 0.093 |
| Depression | 1.18 (1.10–1.27) | <0.001 |
1.08 (1.00–1.18) | 0.049 |
| Anxiety | 1.38 (1.18–1.60) | <0.001 |
1.35 (1.16–1.58) | <0.001 |
| Physical health | ||||
| Musculoskeletal pain | 1.60 (1.49–1.71) | <0.001 |
1.45 (1.34–1.58) | <0.001 |
| Headache or eye pain | 0.89 (0.82–0.97) | 0.009 |
0.98 (0.89–1.07) | 0.607 |
| Fatigue | 1.54 (1.43–1.67) | <0.001 |
1.49 (1.36–1.62) | <0.001 |
| Sickness absence | ||||
| Have experienced | 1.69 (1.41–2.01) | <0.001 |
1.70 (1.43–2.03) | <0.001 |
| Presenteeism | ||||
| Have experienced | 1.77 (1.59–1.98) | <0.001 |
1.82 (1.62–2.04) | <0.001 |
| Health outcomes | Crude model |
Adjusted model |
||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| Self-employed | ||||
| General health | ||||
| Poor | 1.50 (1.19–1.90) | <0.001 |
1.31 (1.00–1.72) | 0.053 |
| Psychological health | ||||
| Sleep disorder | 1.12 (0.90–1.38) | 0.307 | 1.03 (0.82–1.30) | 0.796 |
| Depression | 1.07 (0.92–1.25) | 0.362 | 0.98 (0.83–1.15) | 0.758 |
| Anxiety | 1.19 (0.90–1.58) | 0.214 | 1.17 (0.89–1.55) | 0.264 |
| Physical health | ||||
| Musculoskeletal pain | 1.70 (1.46–1.97) | <0.001 |
1.47 (1.24–1.73) | <0.001 |
| Headache or eye pain | 0.84 (0.70–1.03) | 0.087 | 0.86 (0.71–1.06) | 0.151 |
| Fatigue | 1.49 (1.25–1.78) | <0.001 |
1.37 (1.15–1.63) | <0.001 |
| Sickness absence | ||||
| Have experienced | 2.35 (1.63–3.38) | <0.001 |
2.34 (1.58–3.46) | <0.001 |
| Presenteeism | ||||
| Have experienced | 2.26 (1.77–2.89) | <0.001 |
2.20 (1.71–2.84) | <0.001 |
| Employee | ||||
| General health | ||||
| Poor | 0.89 (0.73–1.08) | 0.238 | 0.97 (0.79–1.20) | 0.779 |
| Psychological health | ||||
| Sleep disorder | 1.07 (0.93–1.24) | 0.350 | 1.13 (0.97–1.31) | 0.116 |
| Depression | 1.15 (1.05–1.26) | 0.002 |
1.11 (1.01–1.22) | 0.025 |
| Anxiety | 1.37 (1.14–1.64) | <0.001 |
1.40 (1.17–1.68) | <0.001 |
| Physical health | ||||
| Musculoskeletal pain | 1.40 (1.29–1.53) | <0.001 |
1.45 (1.32–1.59) | <0.001 |
| Headache or eye pain | 0.90 (0.81–1.00) | 0.051 | 1.00 (0.90–1.11) | 0.983 |
| Fatigue | 1.47 (1.34–1.62) | <0.001 |
1.52 (1.38–1.67) | <0.001 |
| Sickness absence | ||||
| Have experienced | 1.57 (1.28–1.91) | <0.001 |
1.59 (1.30–1.94) | <0.001 |
| Presenteeism | ||||
| Have experienced | 1.65 (1.46–1.87) | <0.001 |
1.75 (1.54–1.99) | <0.001 |
Table 1. Participants’ characteristics according to weekend work status
Values are presented as weighted frequency (%).
Table 2. Prevalence of the health outcomes according to weekend work status
Values are presented as weighted frequency (%).
Table 3. ORs (95% CIs) for health outcomes of weekend workers to non-weekend workers
OR: odds ratio; CI: confidence interval. Adjusted for sex, age, education, monthly income, status of employment, work hours per week.
Table 4. ORs (95% CIs) for health outcomes of weekend workers to non-weekend workers, stratified by status of employment
OR: odds ratio; CI: confidence interval. Adjusted for sex, age, education, monthly income, status of employment, work hours per week.

