
Articles
- Page Path
- HOME > Ann Occup Environ Med > Volume 38; 2026 > Article
- Review Impacts of heat on sleep quality among heat-exposed workers: a systematic review
-
Maarthi Raja1
 , Vidhya Venugopal1,*, D. C. Mathangi2, Suvarna Jyothi Kantipudi3, K. Mahesh Kumar4, Somnath Panda1, Latha Perumal Kamalakkannan1
, Vidhya Venugopal1,*, D. C. Mathangi2, Suvarna Jyothi Kantipudi3, K. Mahesh Kumar4, Somnath Panda1, Latha Perumal Kamalakkannan1 -
Annals of Occupational and Environmental Medicine 2026;38:e3.
DOI: https://doi.org/10.35371/aoem.2026.38.e3
Published online: January 8, 2026
1Faculty of Public Health, Department of Environmental Health Engineering, Sri Ramachandra Institute of Higher Education and Research, Chennai, India
2Department of Mind Body Medicine & Lifestyle Sciences, Sri Ramachandra Faculty of Allied Health Sciences, Sri Ramachandra Institute of Higher Education and Research, Chennai, India
3Department of Psychiatry, Sri Ramachandra Institute of Higher Education and Research, Chennai, India
4Department of Physiology, Government Naturopathy and Yoga Medical College, The Tamil Nadu Dr. M.G.R. Medical University, Chennai, India
- *Corresponding author: Vidhya Venugopal NIHR GHRC NCD-EC, Faculty of Public Health, Department of Environmental Health Engineering, Sri Ramachandra Institute of Higher Education and Research (DU), No. 1, Ramachandra Nagar, Porur, Chennai, Tamil Nadu 600116, India E-mail: vvidhya@ehe.org.in
• Received: October 15, 2025 • Revised: November 26, 2025 • Accepted: December 1, 2025
© 2026 Korean Society of Occupational & Environmental Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,403 Views
- 182 Download
Abstract
- Climate change is intensifying occupational heat exposure, posing risks not only for heat-related illness but also for sleep, which is essential for recovery, safety, and productivity. Heat-exposed workers are highly vulnerable due to prolonged exposure, limited access to cooling, and poor housing. This systematic review aimed to synthesise global evidence on how occupational heat exposure affects sleep quality among workers across different occupations and settings. A systematic review was conducted following Synthesis without Meta-Analysis (SWiM) guidelines. PubMed, Scopus, and Google Scholar were searched (2000–2025) for studies involving adult workers (≥18 years) reporting both heat exposure and sleep outcomes. The review was registered with PROSPERO (ID: CRD420251125735). Of 7,108 records screened, 11 studies met the inclusion criteria. Studies spanned Asia, Australia, North America, and global cohorts. Heat exposure consistently impaired sleep quality and duration. Using Pittsburgh Sleep Quality Index, Actigraphy, and self-reports, common complaints included difficulty falling asleep (64%), restlessness (54%), non-restorative sleep (54%), night sweats (36%), and reduced total sleep time (45%). Night-time temperatures above 25°C and high workplace wet bulb globe temperature values were strongly linked with reduced sleep efficiency and delayed sleep onset. Vulnerable groups included shift workers, petrochemical and steel labourers, women, older adults, and low-income workers in urban heat islands and poorly ventilated housing. Occupational heat exposure disrupts sleep, compounding daytime strain and creating a dual burden for workers. Integrating sleep into heat stress management through cooling interventions, better housing, and revised work–rest schedules is critical for workers well-being in a warming climate.
BACKGROUND
Climate change is intensifying global heat exposure, resulting in more frequent, prolonged, and severe heat waves that pose serious risks to human health, ecosystems, and occupational well-being.1 Globally, about 70% of workers face dangerous heat conditions, causing nearly 23 million injuries and almost 19,000 deaths each year,2,3 defined as environmental conditions where temperature, humidity, and other factors elevate the risk of heat stress.4 Heat-exposed workers, such as those in agriculture, construction, and transportation, face disproportionately high risks due to prolonged exposure to direct sunlight, physically demanding tasks, and limited access to cooling resources.5,6 These risks, caused by heat stress, are expected to intensify in many parts of the world with ongoing climate change.2
Heat stress occurs when the body absorbs or generates more heat than it can dissipate, leading to physiological strain and, if unmitigated, heat-related illnesses such as heat exhaustion and heat stroke.7 Beyond acute outcomes, prolonged or repeated exposure to occupational heat has been linked to chronic conditions such as chronic kidney disease.8,9 However, one important but less studied pathway through which heat affects workers’ health is its impact on sleep quality.
Sleep plays a critical role in physiological recovery, thermoregulation, cognitive performance, and overall well-being.10 Physiologically, the regulation of sleep is closely intertwined with thermoregulation. Prior to sleep onset, core body temperature begins to decline, driven by circadian rhythms, while peripheral vasodilation enhances heat loss through the skin.11 This reduction in core temperature facilitates the transition into non-rapid eye movement sleep, particularly slow-wave sleep, which is restorative for both physical and cognitive functions. Conversely, rapid eye movement (REM) sleep, which is essential for memory consolidation and emotional regulation. High night-time ambient temperatures disrupt normal sleep architecture, reducing slow-wave and REM sleep, delaying sleep onset, and increasing night-time awakenings.12 These disturbances are particularly concerning for heat-exposed workers, who rely on sleep for recovery after physically demanding, heat-intensive labour. Poor sleep exacerbates fatigue, reduces productivity, increases risk of occupational injuries, and contributes to long-term health outcomes such as cardiovascular disease, diabetes, and mental health disorders.13,14
Hence, this inadequate night-time recovery due to sleep disruption combined with intense daytime heat exposure acts as a dual burden for heat-exposed workers in tropical and subtropical regions. Factors such as poor housing, lack of access to cooling, and socioeconomic vulnerability further aggravate the risk.15 For instance, agricultural and construction workers in South and Southeast Asia often live in poorly ventilated homes where ambient night-time temperatures remain high, preventing adequate restorative sleep.16 Moreover, the International Labour Organization has projected that occupational heat stress could reduce global working hours by 2.2% equivalent to 80 million full-time jobs by 2030,17 yet these estimates rarely account for the compounding role of impaired sleep on worker’s productivity and health.
Despite growing recognition of the health implications of climate change and occupational heat, most research has focused on acute heat-related illnesses, hydration, and productivity losses. Far fewer studies have systematically examined how heat exposure specifically affects sleep among heat-exposed workers. Existing evidence is scattered across experimental studies, observational surveys, and wearable-device–based monitoring, but has yet to be synthesised to provide a comprehensive understanding of this critical issue. Therefore, the present systematic review aims to assess and synthesize global evidence on the impact of heat exposure on sleep quality among occupationally heat-exposed workers and related populations, with a focus on (1) identifying differences across urban and rural settings, (2) comparing occupational subgroups, (3) evaluating associations between heat intensity/duration and sleep outcomes, and (4) documenting common sleep-related symptoms and complaints. Insights from this review can inform occupational health guidelines, workplace interventions, and policy measures aimed at mitigating the adverse effects of heat on workers’ sleep and overall well-being.
METHODS
A protocol for this systematic literature review was registered on PROSPERO (ID: CRD420251125735). The search strategy combined keywords using Boolean operators, including terms such as “temperature,” “heat stress,” “sleep quality,” “sleep duration,” and “occupational exposure.” Searches were applied to abstracts and titles, and the reference lists of all included studies and relevant reviews were hand-searched for additional records. This strategy ensured both sensitivity and specificity in capturing relevant literature. Prior to final synthesis, all searches were re-run to include the most current research.
Following the article search, a two-step screening process was undertaken, consisting of title/abstract screening followed by full-text screening. The search, screening, and selection procedures were conducted in accordance with the Preferred Reporting Items for Systematic Reviews (PRISMA).18 All retrieved articles were exported into the Covidence software. Two independent reviewers (MR and SP) conducted title and abstract screening, followed by full-text screening, while a third reviewer (VV) resolved conflicts between the two reviewers.
The extracted data was summarized in tabular form with the following column headings: author, year, study location, study title, study purpose, study design, sample population, sample size, primary outcomes, methods of measuring outcomes, comparators (if any), and summary of key findings. Study authors were contacted when gaps or inconsistencies in the reported data were identified. Data from all the included articles are presented in the summary of findings tables. For outcomes reported as continuous data, the review will present mean values or differences in mean scores across study groups wherever possible.
We assessed the methodological quality of the included studies using validated tools tailored to each study design. For cohort, cross-sectional, and longitudinal studies, we applied the Joanna Briggs Institute (JBI) Critical Appraisal Checklists appropriate for each design19 (Supplementary Tables 1–3). Two reviewers (MR and SP) independently assessed all studies using the JBI risk of bias checklist. A third reviewer (VV) resolved any disagreements when necessary.
Ethical clearance was obtained from the Institutional Ethics Committee (IEC) of Sri Ramachandra Institute of Higher Education and Research (IEC-NI/25/04/103/78).
RESULTS
The database search retrieved a total of 7,108 references for screening. After manual and automated duplicate removal (n = 2,766), 4,342 unique records remained. Title and abstract screening excluded 4,300 studies that did not meet the inclusion criteria. Forty-two full-text articles were assessed for eligibility, of which 31 were excluded for reasons including: no mention of heat exposure (n = 16), wrong exposure (n = 3), no exposure to heat (n = 2), wrong outcomes (n = 2), wrong study design (n = 2), excluded work location (n = 1), wrong comparator (n = 1), and wrong patient population (n = 4). Ultimately, 11 studies were included in the systematic review (Fig. 1).
Among the eleven included studies, the majority employed cross-sectional designs (n = 6),20-24 while three were observational or cohort studies with wearable-based measures12,25-27 and one applied predictive modelling using machine learning across large-scale global survey datasets.24
Sample sizes varied considerably across the included studies, reflecting differences in study design and feasibility. Smaller occupational and field-based investigations enrolled fewer participants, such as 19 underground miners26 and 30 low-income residents monitored with wearable sensors,25 allowing for detailed physiological and environmental assessments but limiting generalisability. In contrast, national cross-sectional surveys engaged much larger samples, including 2,822 Korean workers28 and 29,213 employees from the Korean Working Conditions Survey.29 Global panel datasets reached even broader scales, such as 47,628 adults contributing nearly 7 million nightly sleep records across 68 countries.27 Finally, advanced modelling work among petrochemical workers analysed over 2,300 participants and incorporated machine/deep learning with more than 1.5 million data points,24 enhancing external validity while relying on indirect exposure estimation and self-reported sleep indicators.
Geographic distribution of the included studies was largely concentrated in Asia, where vulnerability to rising temperatures and occupational heat stress is well-documented. Several studies originated from Korea,28,29 China,23,24 and Indonesia,21 alongside evidence from Australia.20 North American contributions included a U.S. study on low-income urban residents25 and Canadian fieldwork among underground miners.26 Broader global contexts were captured by,27 who analysed over 7 million nightly sleep records across 68 countries. Collectively, this distribution ensured representation of both tropical and temperate settings, though Asian studies dominated the evidence base (Fig. 2).
Populations studied included heat-exposed workers, such as petrochemical employees,23,24 steel rolling mill workers,21 and heat-exposed workers identified through compensation records.30 Broader groups encompassed general employees, including the labourers across occupational sectors in Australia,20 shift-working underground miners,26 and community-based participants who are working outdoors and are exposed to urban heat in Houston.25 Large-scale surveys captured the general Korean workforce,28,29 while global data were drawn from multi-country cohorts covering 68 nations.27
Heat exposure was assessed through multiple approaches. Wet bulb globe temperature (WBGT) indices and workplace climate measures were used in occupational studies,21,23,30 while ambient or night-time temperature monitoring with wearable sensors provided person-specific measures.25,27 Several investigations relied on self-reported workplace exposures or heat-related discomfort.20,24,28,29
Sleep outcomes were captured through both subjective and objective methods. The Pittsburgh Sleep Quality Index (PSQI) was the most frequently applied tool,20,21,23,28,29 offering a validated though self-reported measure of sleep quality. Actigraphy was employed in field and global studies to objectively assess total sleep time (TST) and efficiency,25-27 while self-reported sleep indicators20,24 and sleep diaries26 provided complementary insights into timing, duration, and disturbances.
Heat exposure consistently worsened sleep outcomes across both subjective and objective measures. WBGT-based occupational studies showed strong associations: severe high-temperature exposure increased sleep disturbance in Korean workers (odds ratio [OR]: 3.09 in men; OR: 3.30 in women), while petrochemical workers in China also showed elevated risk (OR: 1.77), with additional effects from long working hours (OR: 1.74) and occupational stress (OR: 2.67). Objective studies demonstrated clear heat-related sleep loss. Global accelerometer data showed that each 1°C rise in night-time temperature reduced sleep by ~5–10 minutes, with older adults and women most affected. Very hot nights (>30°C) cut sleep by ~14.1 minutes, and nights above 25°C increased insufficient sleep (<7 hours) by ~3.5 percentage points. Wearable-sensor data from low-income U.S. adults showed a β = −2% decline in sleep efficiency per 1°C, mitigated by air conditioning. Other occupational studies, including steel and mining sectors, reported significant associations between heat, sleep quality, and fatigue (p = 0.031–0.047) despite lacking OR/RR estimates (Table 1).12,20,21,23-30
Heat-exposed workers experienced substantial reductions in TST (30–40 minutes) and sleep efficiency, frequently reporting difficulty falling asleep during hot nights.25 Steel workers exposed to WBGT ranges of 28–32°C showed poor PSQI scores and frequent night sweats and fatigue, with workplace noise exacerbating these effects.21 Petrochemical workers reported elevated PSQI scores, restlessness, and insomnia, with fatigue mediating the relationship between prolonged WBGT exposure and poor sleep.23,24 Factory workers, particularly those in Malaysia, experienced non-restorative sleep due to the combined impact of indoor heat and shift-related demands.28 Similarly, general shift workers in Korea exhibited high rates of disturbed sleep (49.9%), reflecting poor recovery and circadian disruption.28,29 Labourers exposed regularly to heat, noise, and poor air quality had significantly higher odds of insufficient sleep (OR: 3.15; 95% confidence interval [CI]: 1.29–7.66) and delayed sleep timing (“Owl” chronotype; OR: 3.47; 95% CI: 1.24–9.71).20 Collectively, these findings suggest that physically demanding, heat-intensive occupations pose the greatest sleep-related risks, with overlapping exposures such as noise, chemicals, and shift schedules further exacerbating adverse outcomes (Table 2).26,27,29
Four studies assessed the impact of heat on sleep across urban and rural or semi-urban contexts (Table 3).23,25,29,30 In Houston,25 showed that urban low-income residents experienced significant reductions in sleep efficiency, with risks exacerbated by poor housing quality and infrequent air conditioning use, highlighting the urban heat island effect. In Korea,29 reported that high workplace temperatures were strongly associated with self-reported sleep disturbances, although the study did not directly contrast urban and rural groups; industrial and urban workers appeared to be at greater risk.23 Examining petrochemical workers in China, the study found that high WBGT exposures were associated with poor PSQI scores, but no significant differences were observed between rural-born and urban-born workers after propensity score matching. Finally, Park et al.29 identified that 78.7% of occupational heat illness cases occurred following tropical nights, underscoring how elevated nocturnal temperatures, particularly in urban areas, contribute to both poor sleep and heightened heat-related health risks. The urban heat island effect intensified risks in metropolitan regions.27
Across the 11 included studies, several heat-related sleep complaints were consistently reported. The most frequent was difficulty falling asleep, observed in 64% of studies, particularly among petrochemical workers, factory workers, and shift workers exposed to high workplace temperatures or tropical nights.23,24,28-30 Restlessness (54%) and non-restorative sleep (54%) were also common, with petrochemical workers and general employees frequently citing poor recovery and insomnia under chronic WBGT exposure and long working hours.20,23,26 Night sweats (36%) were particularly noted among steel workers and underground miners working under WBGT ranges of 28–32°C and humid environments.21,26 Finally, reduced TST (45%) was documented in both occupational and population-wide studies, with wearable-based findings.25,27 Taken together, these findings highlight that heat exposure most often impairs sleep initiation and continuity, while also exacerbating fatigue through reduced sleep duration and quality (Table 4).
Quality appraisal using the JBI tool indicated that all studies were of good methodological quality. Each study clearly described its participants and settings, used appropriate outcome measures (PSQI, actigraphy, polysomnography, sleep diaries), and applied reliable statistical analyses.
DISCUSSION
This systematic review provides evidence that occupational and environmental heat exposure is consistently associated with poor sleep outcomes among heat-exposed workers across diverse industrial and occupational settings. The synthesis of 11 cross-sectional and cohort studies from Asia, Australia, North America and global countries indicates that exposure to high temperatures, whether measured objectively through WBGT, indoor/outdoor recordings, or self-reported perceptions of heat, is negatively related to sleep quality, duration, and restfulness. These effects were reported across various occupational groups, including petrochemical workers, steel mill labourers, miners, and heat-exposed workers, highlighting the pervasiveness of the problem in both industrial and service sectors.
Across studies, heat exposure was strongly linked to self-reported insomnia, difficulty initiating and maintaining sleep, excessive sweating at night, and poor sleep efficiency as measured by validated scales such as the PSQI.21,23,28 Objective measures, including Actigraphy and Polysomnography, confirmed that higher ambient or workplace temperatures shortened TST and increased wake after sleep onset.20,26 Importantly, studies using WBGT in petrochemical settings showed that workers exposed to “high” or “very high” heat loads were significantly more likely to report non-restorative sleep and fatigue.23,24 These results align with physiological evidence demonstrating that thermoregulatory strain disrupts sleep architecture by reducing slow-wave and REM sleep.31
Although the present review focuses on heat-exposed workers, its findings align with broader epidemiological studies that link ambient heat to sleep disruption in general populations. Large-scale investigations using wearable devices and survey data have demonstrated that each 1°C rise in night-time temperature reduces sleep duration by 7–14 minutes, with greater losses in vulnerable groups such as the elderly and low-income populations.12,27,32 The congruence between occupational and community-level findings suggests that heat is a universal risk factor for sleep loss, but heat-exposed workers face amplified exposure due to extended periods in hot environments, often with limited access to cooling strategies. Reviews of occupational heat strain have already documented increased risks of dehydration, renal dysfunction, accidents, and reduced productivity,5,33 yet the contribution of sleep disturbance to these adverse outcomes has received little systematic attention. This review, therefore, fills an important gap by consolidating heat-exposed workers-focused evidence on sleep disruption.
Multiple mechanisms likely explain the heat–sleep relationship in heat-exposed workers. Elevated ambient temperatures impair the body’s ability to achieve the nocturnal drop in core temperature required for sleep initiation, leading to prolonged sleep latency and fragmented sleep.31 Heat-exposed workers exposed to heat during the day may also experience delayed recovery, as sustained hyperthermia and dehydration compromise night-time thermoregulation. Shift workers, who already face circadian misalignment, are particularly vulnerable when high night-time temperatures coincide with recovery periods.29,30 Further, psychosocial stressors such as fear of heat-related illness, fatigue, or inadequate housing conditions (e.g., lack of air conditioning or ventilation) can exacerbate sleep disruption.
The included studies demonstrated good overall methodological quality according to the JBI assessment tool. However, several limitations should be noted. Heat exposure measurement methods varied considerably across studies. Some studies used objective measurements such as WBGT and indoor environmental monitoring,23,24 while others relied on participants' self-reported perceptions of workplace heat.21,28 This variation in exposure assessment methods may have introduced measurement bias into the findings. Confounding adjustment was inconsistent; only a minority of studies controlled for humidity, air conditioning access, or socioeconomic status, despite these being critical determinants of both heat exposure and sleep. Moreover, the predominance of cross-sectional designs limits causal inference. Very few studies assessed lagged or cumulative heat effects on sleep, which may be important given the delayed recovery patterns reported in experimental research.31 It is also important to recognize that sleep disturbance is primarily an indoor phenomenon and may be influenced by additional non-thermal factors such as social stress, medication use, comorbid health conditions, and indoor environmental characteristics like ventilation, noise, and crowding.11,34 Current studies have not consistently standardised populations to isolate heat as the sole determinant of disturbed sleep. For instance, medications that alter thermoregulation or underlying health vulnerabilities may exacerbate heat-related sleep disruptions.35 Furthermore, social stress and poor interpersonal environments are increasingly recognised as critical determinants of sleep health.36 While heat exposure has been linked to impaired cardiovascular outcomes and altered recovery during sleep,37 confounding from non-thermal factors is rarely addressed. Incorporating broader confounder adjustment and standardised study designs would enhance causal inference and help delineate the independent contribution of heat exposure to sleep outcomes, especially among working populations where sleep quality is crucial for cognitive performance and occupational safety.36 These gaps underscore the need for stronger methodological rigor in future occupational sleep research.
Evidence from the included studies highlights several directions for strengthening heat–sleep management among workers. Current regulatory guidelines—such as those from National Institute for Occupational Safety and Health, American Conference of Governmental Industrial Hygienists38,39, and the Indian Factories Act40 primarily focus on acute heat strain, metabolic workload, and WBGT thresholds, but none explicitly incorporate sleep-related outcomes. This gap is important because multiple studies in our review link elevated ambient temperatures to reduced sleep duration and efficiency. These findings suggest that considering sleep within heat-exposure frameworks may improve workers safety and recovery.
Studies included in this review also point to specific factors that may inform adaptation measures. For example, actigraphy-based studies12,25 demonstrate consistent reductions in sleep efficiency with rising night-time temperatures, while research comparing indoor and outdoor exposure indicates that indoor heat may have stronger effects on sleep quality.27 Furthermore, included studies highlight gender-based differences, with women reporting higher heat-related symptoms.12,29 Such evidence underscores the need for targeted monitoring of vulnerable groups, including heat-exposed workers, women, older adults, and informal-sector workers in low- and middle-income settings.25
Broader policy recommendations such as adjusting work schedules to cooler hours, improving ventilation in worker housing, enhancing shaded rest areas,5 and incorporating relaxation or cooling strategies are suggested as potential avenues for future intervention.33 While not all of these measures were directly tested in the included studies, they align with established heat-management guidelines and emerging evidence linking thermal environments to sleep disruption. We have therefore clarified which points are directly supported by the studies in this review and which represent broader implications requiring further evaluation.
The study provides comprehensive evidence by synthesising 11 studies across diverse geographic regions (Asia, Australia, North America and global countries) and multiple occupational groups, including petrochemical workers, steel mill labourers, miners, and heat-exposed workers. The multi-dimensional approach combines objective heat exposure measures (WBGT, temperature monitoring) with subjective assessments, validated sleep tools (PSQI), and both self-reported and objective sleep measures (actigraphy, polysomnography). Importantly, the review addresses a significant research gap by focusing on worker-specific sleep disruption evidence, extending beyond traditional occupational heat research that emphasises acute strain and productivity. The study establishes a strong theoretical foundation by aligning its findings with broader epidemiological evidence and providing plausible physiological mechanisms that explain the heat-sleep relationship in occupational settings.
Limitations include methodological inconsistencies, such as a wide variation in exposure assessment methods, with some studies using objective measures while others relying on self-reported perceptions, which may introduce bias. Only a minority of studies controlled for critical confounding factors such as humidity, air conditioning access, or socioeconomic status. The predominance of cross-sectional designs limits causal inference, and few studies assessed lagged or cumulative heat effects despite evidence of delayed recovery patterns. The review's scope was limited by insufficient longitudinal studies, inadequate attention to vulnerable populations (agricultural workers, women, and informal sector workers in low- and middle-income countries), and restricted geographic representation. A meta-analysis was not feasible due to the significant heterogeneity among the included studies, which varied widely in methodology, design, and outcomes. These limitations underscore the need for longitudinal studies, improved confounding control, diverse populations, and interventional research to develop effective workplace solutions.
CONCLUSIONS
This systematic review demonstrates that occupational heat exposure significantly impairs sleep quality across heat-exposed workers, establishing sleep disturbance as an under recognised consequence of workplace heat stress extending beyond immediate injuries to affect broader workers’ well-being and performance. Heat-induced sleep disruption creates cascading health effects, including impaired cognition, reduced immunity, and increased accident risk. For vulnerable workers in physically demanding jobs, sleep disruption compounds existing health risks and perpetuates fatigue cycles. As climate change intensifies extreme heat globally, this intersection becomes increasingly urgent. Sleep-deprived workers show reduced productivity and increased healthcare costs, creating both health and economic concerns. Protecting workers’ sleep must become essential to heat safety programs, requiring a shift from reactive heat illness prevention to proactive sleep health protection. This includes integrating sleep assessment into occupational guidelines, developing interventions addressing daytime heat exposure and night-time recovery, and incorporating sleep considerations into heat action plans.
Future research should focus on evidence-based interventions, cooling strategies for work and rest periods, and establishing sleep quality as a standard heat stress metric. Only through comprehensive approaches can we adequately protect worker health and productivity in our warming world.
Abbreviations
AC
air conditioner
CI
confidence interval
DL
deep learning
JBI
Joanna Briggs Institute
KWCS
Korean Working Conditions Survey
MD
mean difference
ML
machine learning
OR
odds ratio
PSQI
Pittsburgh Sleep Quality Index
REM
rapid eye movement
RR
risk ratio
SE
sleep efficiency
TST
total sleep time
WASO
wake after sleep onset
WBGT
wet bulb globe temperature
-
Competing interests
No potential conflict of interest relevant to this article was reported.
-
Author contributions
Conceptualization: Raja M, Venugopal V. Data curation: Panda S, Kamalakkannan LP, Mathangi DC, Kantipudi SJ, Kumar KM. Formal analysis: Raja M. Investigation: Raja M, Panda S, Kamalakkannan LP. Methodology: Raja M, Venugopal V. Project administration: Raja M. Supervision: Raja M, Venugopal V. Validation: Venugopal V. Writing - original draft: Raja M, Panda S, Kamalakkannan LP. Writing - review & editing: Venugopal V.
-
Acknowledgments
The authors highly acknowledge and thank the Department of Environmental Health Engineering, Sri Ramachandra Institute of Higher Education and Research, Chennai, for providing us with this platform for carrying out the work. The authors also acknowledge the NIHR-Global Health Research Centre award scheme (Grant number GHRC for NCDs and EC: NIHR203247), using UK international development funding from the UK Government to support global health research. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the UK government.
NOTES
SUPPLEMENTARY MATERIAL
Supplementary Table 1.
Critical appraisal of eligible analytical cross-sectional study.
Supplementary Table 2.
Critical appraisal of eligible cohort study.
Supplementary Table 3.
Critical appraisal of eligible prevalence study.
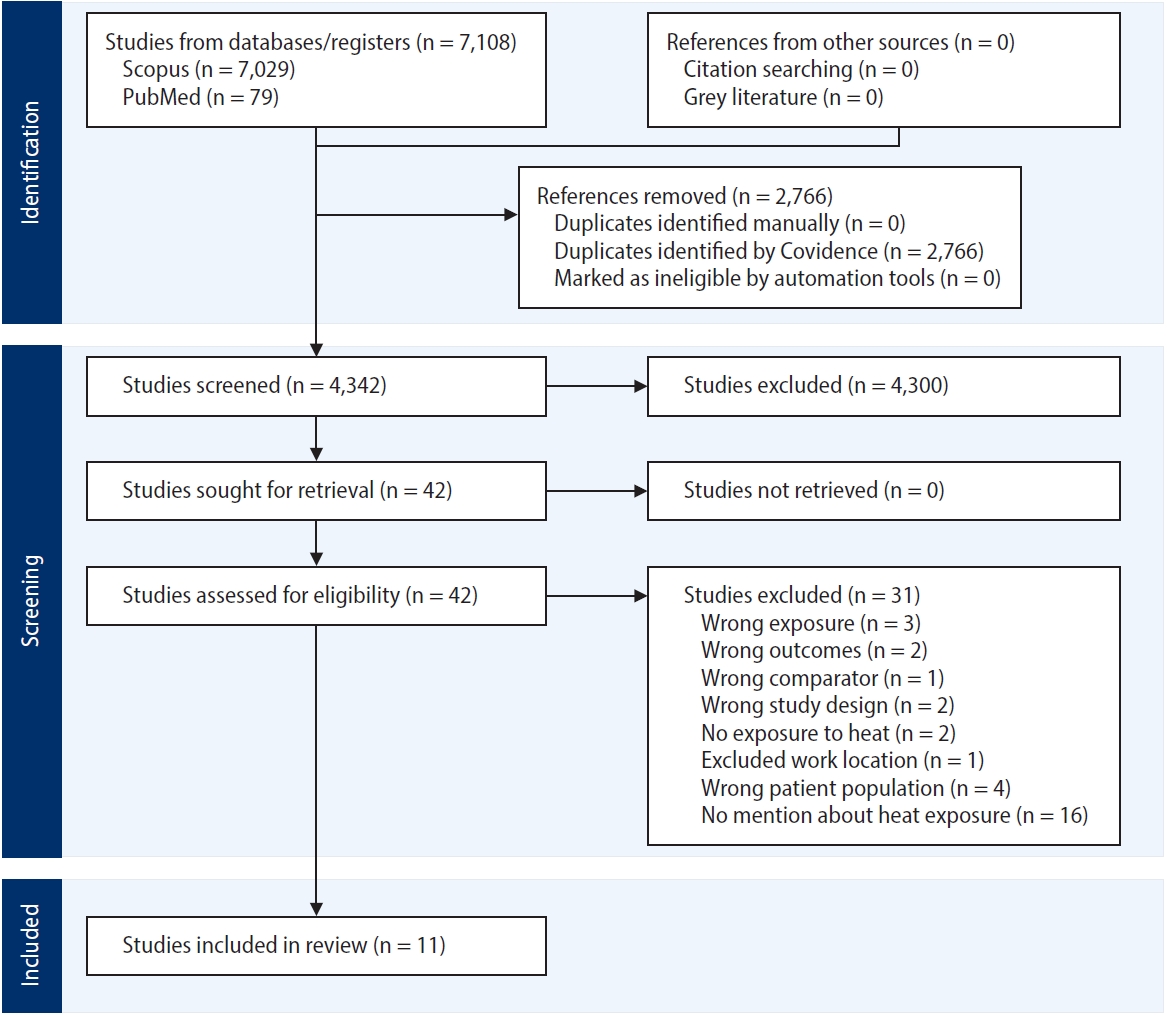
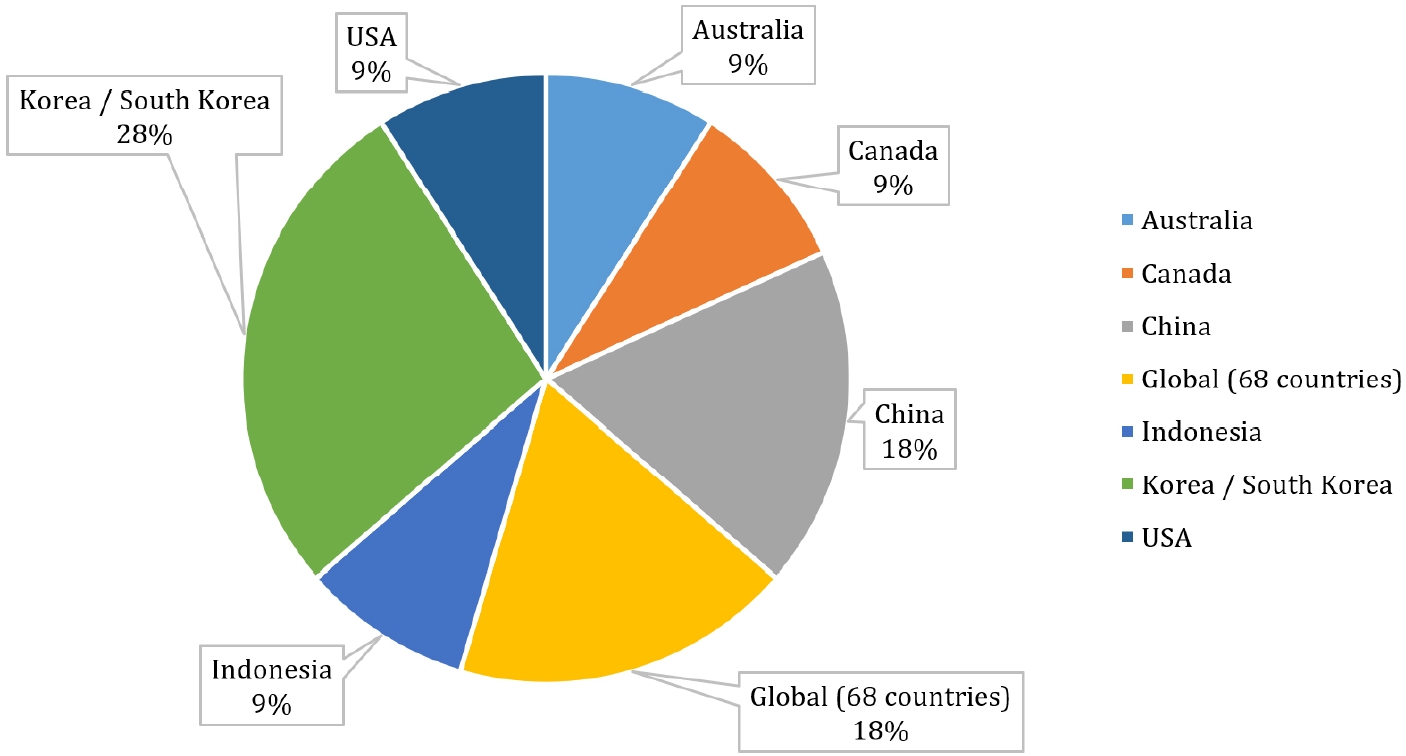
Table 1.
Overview of included studies
| Study | Country | Study design | Sample size | Population (occupation/setting) | Exposure measure (WBGT, temperature) | Sleep measure (PSQI, actigraphy, diary) | Key finding | Effect estimate (OR/RR/β/MD) |
|---|---|---|---|---|---|---|---|---|
| Wu et al. (2024)23 | China | Cross-sectional | 952 | Petrochemical workers (enterprise) | WBGT | PSQI, total score; cutoff = 7 used to classify “sleep disorders” | 41.9% Prevalence; risk higher with >40 hour/week, heat, stress | No OR/RR/β/MD reported |
| Minor et al. (2022)27 | Global (68 countries) | Observational (wearable + climate data) | 7M+ sleep records | Workers and general population (68 countries) | Ambient temperature | Actigraphy (wearable fitness bands), total night-time sleep (minutes); sleep onset/offset; and short-sleep binary indicators using standard thresholds <7 hours, <6 hours, <5 hours | Night-time temp >25°C reduces sleep, increases insufficient sleep risk | MD: 1°C rise → ~5–10 minutes loss of sleep (varies by age/sex) |
| Hyun (2024)28 | Korea | National cross-sectional survey | 2,822 | General workforce (nationwide) | Not mentioned about exposure measurement | PSQI (Korean version); cut-off = 8.5 or more denotes presence of sleep disturbance | 49.9% Prevalence; risk higher with two-shift work, >53 hour/week, cold/heat symptoms | Paper reports associations between CHPI domains and sleep |
| Cheong and Gaynanova (2024)25 | USA | Observational (wearable sensing, mixed models) | 30 | Low-income, predominantly Black adults, Houston | Ambient temperature | Actigraphy (GENEActiv: sleep efficiency, TST) | 1°C Rise → ~2% decrease in sleep efficiency; AC mitigated effects | β = −2% sleep efficiency per 1°C increase (AC reduces effect) |
| Legault et al. (2017)26 | Canada | Field study, longitudinal (28–30 days) | 19 | Male underground miners, rotating shifts | Ambient conditions + WBGT (temp, humidity) | Actigraphy (TST, SE, WASO) + PSQI + sleep logs | Poor sleep vs. norms; 61% poor sleepers; degraded attention during night shifts under heat stress | No OR/RR/β/MD reported |
| Park et al. (2022)29 | Korea | Cross-sectional survey (KWCS) | 29,213 | Paid Korean workers (varied industries) | WBGT | Self-report (difficulty falling/maintaining sleep, fatigue) | Severe high-temperature exposure and sleep disturbance (OR: 3.09 in men; 3.30 in women); dose-response effect | OR (severe high temperature): men = 3.09 (95% CI: 2.69–3.56); women = 3.30 (95% CI: 2.81–3.87) |
| Magee et al. (2019)20 | Australia | Cross-sectional survey + Latent Class Analysis (LCA) | 542 employees (aged 18–60) | Australian employees, various sectors | Didn’t mention heat exposure measurement | Bed/wake times, sleep duration (work vs. non-work days), perceived sleep quality | Regular exposure to environmental stressors was linked to insufficient sleep (OR: 3.15) and “owls” (late sleepers; OR: 3.47) | ORs: Regular exposure class associated with insufficient sleep (OR: 3.15; 95% CI: 1.29–7.66) and with owls (OR: 3.47; 95% CI: 1.24–9.71) |
| Rasyid (2023)21 | Indonesia | Cross-sectional | 31 | Rolling mill steel industry workers | Work climate (WBGT) | PSQI, total score; cut off <5 = good sleep; ≥5 = poor sleep (they state PSQI <5 good, >5 poor) | Physical workload (p = 0.031), poor sleep quality (p = 0.047), hot climate (p = 0.002), and high noise (p = 0.009) were significantly associated with work fatigue | No OR/RR/β reported; associations only by p-values: physical workload vs. fatigue (p = 0.031) and sleep quality vs. fatigue (p = 0.047) |
| Minor et al. (2020)12 | 68 Countries worldwide | Observational, panel data analysis | 47,628 Adults, ~7 million nightly sleep records | Workers and general population (accelerometer users) | Night-time outdoor temperature (weather station data) | Wrist-worn accelerometers (sleep duration, onset, offset). Insufficient sleep <7 hours. Heat-associated deviations analyzed in minutes | Hotter nights shortened sleep, especially in older adults and women | Effect estimates (β/MD/percentage-point): Very warm nights (>30°C) reduced sleep by ~14.1 minutes (CI: −17.6 to −10.6). Nights >25°C increased the probability of sleeping <7 hours by ~3.5 percentage points compared with baseline 5–10°C nights |
| Park et al. (2017)30 | South Korea | Case-series using compensation records | 47 Compensated cases (2010–2014) | Heat-exposed workers (construction, cleaning, agroforestry) | WBGT (estimated from meteorological data), heat wave, tropical night | Lack of sleep provided by tropical nights | 95.7% Cases occurred when WBGT exceeded threshold; 61.7% during heat waves | No OR/RR; 95.7% of heat-related cases occurred above WBGT threshold; 61% during heat waves |
| Zhang et al. (2024)24 | China | Cross-sectional survey with ML/DL modelling | 2,393 Valid participants | Petrochemical workers, Fujian Province | Self-reported “temperature discomfort” using a 6-item scale assessing how high temperatures affected work efficiency | Sleep quality and sleep onset difficulty (questionnaire) | 18.0% reported poor sleep; poor sleep linked with higher productivity loss | High temperature exposure (OR: 1.77; 95% CI: 1.12–2.81), weekly >40 hours (OR: 1.74; 95% CI: 1.09–2.82), occupational stress (OR: 2.67; 95% CI: 1.89–3.80) |
WBGT: wet bulb globe temperature; PSQI: Pittsburgh Sleep Quality Index; OR: odds ratio; RR: risk ratio; MD: mean difference; CHPI: Composite Heat Exposure Index; TST: total sleep time; AC: air conditioner; SE: sleep efficiency; WASO: wake after sleep onset; KWCS: Korean Working Conditions Survey; CI: confidence interval; ML: machine learning; DL: deep learning.
Table 2.
Summary of the sleep performance among different occupational settings
Table 3.
Sleep quality among urban and rural workers
| Study | Setting | Environmental measure | Duration/Intensity | Sleep outcomes (PSQI, TST, SE) | Main findings |
|---|---|---|---|---|---|
| Cheong and Gaynanova (2024)25 | Urban, Houston, low-income housing | Person-specific ambient temperature; AC use; outdoor temperature (25–38°C) | 14 Days of continuous monitoring | Sleep efficiency ↓ 2% per °C rise | Vulnerable urban residents (low AC use, poor housing) had worse sleep |
| Park et al. (2022)29 | National (urban and rural) | Self-report workplace temperature (high/low) | Chronic workplace exposures | Sleep disturbance (self-report) | High-temp workplaces (often industrial/urban) had a stronger association with poor sleep |
| Wu et al. (2024)23 | Petrochemical enterprise (Hainan, China) | WBGT, workplace monitoring | Chronic high temp (≥25°C WBGT) | PSQI | Rural-born vs. urban-born workers |
| Park et al. (2017)30 | Korean heat-exposed workers (construction, cleaning, agroforestry) | WBGT, tropical night (>25°C), heat wave (≥33°C for 2+ days) | Acute heat illness episodes (2010–2014) | Lack of sleep inferred from tropical nights | 78.7% of heat-illness cases followed tropical nights, suggesting urban night heat worsens sleep and heat risk |
Table 4.
Reported symptoms/complaints
| Symptom/Complaint | No. of studies reporting | % of total (n = 11) |
|---|---|---|
| Difficulty falling asleep | 7 | 64 |
| Night sweats | 4 | 36 |
| Restlessness | 6 | 54 |
| Non-restorative sleep | 6 | 54 |
| Reduced total sleep time | 5 | 45 |
- 1. Intergovernmental Panel on Climate Change. Global Warming of 1.5°C: An IPCC Special Report on the Impacts of Global Warming of 1.5°C above Pre-industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty. Geneva, Switzerland: Intergovernmental Panel on Climate Change; 2018.
- 2. World Meteorological Organization. The Global Climate 2011-2020: A Decade of Accelerating Climate Change. Geneva, Switzerland: World Meteorological Organization; 2023.
- 3. World Health Organization. Climate change and workplace heat stress: technical report and guidance. https://www.who.int/publications/i/item/9789240099814. Updated 2025. Accessed September 3, 2025 ArticlePubMedPDF
- 4. Kjellstrom T, Briggs D, Freyberg C, Lemke B, Otto M, Hyatt O. Heat, human performance, and occupational health: a key issue for the assessment of global climate change impacts. Annu Rev Public Health 2016;37:97–112.ArticlePubMed
- 5. Flouris AD, Dinas PC, Ioannou LG, Nybo L, Havenith G, Kenny GP, et al. Workers' health and productivity under occupational heat strain: a systematic review and meta-analysis. Lancet Planet Health 2018;2(12):e521–31.ArticlePubMed
- 6. Kjellstrom T, Freyberg C, Lemke B, Otto M, Briggs D. Estimating population heat exposure and impacts on working people in conjunction with climate change. Int J Biometeorol 2018;62(3):291–306.ArticlePubMedPDF
- 7. Parson K. Human Thermal Environments: The Effects of Hot, Moderate, and Cold Environments on Human Health, Comfort, and Performance. 3rd ed. Boca Raton, FL: CRC Press; 2014.
- 8. Glaser J, Hansson E, Weiss I, Wesseling C, Jakobsson K, Ekstrom U, et al. Preventing kidney injury among sugarcane workers: promising evidence from enhanced workplace interventions. Occup Environ Med 2020;77(8):527–34.ArticlePubMedPMC
- 9. Johnson RJ, Sanchez-Lozada LG, Newman LS, Lanaspa MA, Diaz HF, Lemery J, et al. Climate change and the kidney. Ann Nutr Metab 2019;74 Suppl 3:38–44.ArticlePubMedPDF
- 10. Medic G, Wille M, Hemels ME. Short- and long-term health consequences of sleep disruption. Nat Sci Sleep 2017;9:151–61.ArticlePubMedPMCPDF
- 11. Krauchi K, Deboer T. The interrelationship between sleep regulation and thermoregulation. Front Biosci (Landmark Ed) 2010;15(2):604–25.ArticlePubMed
- 12. Minor K, Bjerre-Nielsen A, Jonasdottir SS, Lehmann S, Obradovich N. Ambient heat and human sleep. http://arxiv.org/abs/2011.07161. Updated 2020. Accessed September 3, 2025.
- 13. Ding R, Wang Y, Yu Y, Meng X, Gong Q, Tang Y, et al. Effectiveness of a multifaceted intervention (TEMP) for prevention of occupational heat-related illness among outdoor workers in the power grid industry: a cluster randomized controlled trial. Environ Health Perspect 2025;133(1):17001.ArticlePubMedPMC
- 14. Grandner MA. Sleep, health, and society. Sleep Med Clin 2022;17(2):117–39.ArticlePubMed
- 15. Gong L, Wang L, Hu R, Lu X, Sun Y, Zhang S, et al. Identification of unique ecosystem service bundles in farmland: a case study in the Huang-Huai-Hai Plain of China. J Environ Manage 2024;370:122516.ArticlePubMed
- 16. Sahu S, Sett M, Kjellstrom T. Heat exposure, cardiovascular stress and work productivity in rice harvesters in India: implications for a climate change future. Ind Health 2013;51(4):424–31.ArticlePubMed
- 17. International Labour Organization. Increase in heat stress predicted to bring productivity loss equivalent to 80 million jobs. http://www.ilo.org/global/about-the-ilo/newsroom/news/WCMS_711917/lang--en/index.htm. Updated 2019. Accessed September 15, 2023.
- 18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev 2021;10:89.PubMedPMC
- 19. Hilton M. JBI Critical appraisal checklist for systematic reviews and research syntheses. J Can Health Libr Assoc 2024;45(3):180–3.PMC
- 20. Magee C, Gopaldasani V, Bakand S, Coman R. The physical work environment and sleep: a latent class analysis. J Occup Environ Med 2019;61(12):1011–8.PubMed
- 21. Rasyid MF. Relationship between physical workload, sleep quality, work climate, and noise level with work fatigue in rolling mill workers in Sidoarjo steel industry. Indones J Public Health 2023;17(2):319–30.ArticlePDF
- 22. Park JS, Park EK, Kim HK, Choi GS. Prevalence and risk factors of occupational skin disease in Korean workers from the 2014 Korean Working Conditions Survey. Yonsei Med J 2020;61(1):64–72.ArticlePubMedPMCPDF
- 23. Wu Q, Fan S, Zhou B, Lu C, Zhang N, Su Z, et al. Relationship between occupational factors and sleep disorders among petrochemical workers on Hainan Island, South China: a cross-sectional study. Int J Occup Med Environ Health 2024;37(6):591–601.ArticlePubMedPMCPDF
- 24. Zhang Y, Chen Y, Su Q, Huang X, Li Q, Yang Y, et al. The use of machine and deep learning to model the relationship between discomfort temperature and labor productivity loss among petrochemical workers. BMC Public Health 2024;24(1):3269.ArticlePubMedPMCPDF
- 25. Cheong SM, Gaynanova I. Sensing the impact of extreme heat on physical activity and sleep. Digit Health 2024;10:20552076241241509.ArticlePubMedPMCPDF
- 26. Legault G, Clement A, Kenny GP, Hardcastle S, Keller N. Cognitive consequences of sleep deprivation, shiftwork, and heat exposure for underground miners. Appl Ergon 2017;58:144–50.ArticlePubMed
- 27. Minor K, Bjerre-Nielsen A, Jonasdottir SS, Lehmann S, Obradovich N. Rising temperatures erode human sleep globally. One Earth 2022;5(5):534–49.Article
- 28. Hyun MK. General worker's sleep disturbances and the degree of cold-heat symptoms: a national cross-sectional survey. J Pharmacopuncture 2024;27(3):199–210.ArticlePubMedPMC
- 29. Park I, Kim S, Kim Y, Yun B, Yoon JH. Association between physical risk factors and sleep disturbance among workers in Korea: the 5th Korean Working Conditions Survey. Sleep Med 2022;100:157–64.ArticlePubMed
- 30. Park J, Kim Y, Oh I. Factors affecting heat-related diseases in outdoor workers exposed to extreme heat. Ann Occup Environ Med 2017;29:30.ArticlePubMedPMCPDF
- 31. Okamoto-Mizuno K, Mizuno K. Effects of thermal environment on sleep and circadian rhythm. J Physiol Anthropol 2012;31(1):14.ArticlePubMedPMCPDF
- 32. Obradovich N, Migliorini R, Mednick SC, Fowler JH. Nighttime temperature and human sleep loss in a changing climate. Sci Adv 2017;3(5):e1601555.ArticlePubMedPMC
- 33. Xiang J, Bi P, Pisaniello D, Hansen A. The impact of heatwaves on workers' health and safety in Adelaide, South Australia. Environ Res 2014;133:90–5.ArticlePubMed
- 34. Bragazzi NL, Garbarino S, Puce L, Trompetto C, Marinelli L, Curra A, et al. Planetary sleep medicine: studying sleep at the individual, population, and planetary level. Front Public Health 2022;10:1005100.ArticlePubMedPMC
- 35. Nabeel I, Caraballo-Arias Y, Perkison WB, McCarthy RB, Saberi P, Berenji M, et al. Proposed mitigation and adaptation strategies related to climate change: guidance for OEM professionals. J Occup Environ Med 2021;63(9):e650–6.ArticlePubMed
- 36. Lo JC, Ong JL, Leong RL, Gooley JJ, Chee MW. Cognitive performance, sleepiness, and mood in partially sleep deprived adolescents: the need for sleep study. Sleep 2016;39(3):687–98.ArticlePubMedPMC
- 37. Ashe N, Wozniak S, Conner M, Ahmed R, Keenan O, Demetres MR, et al. Association of extreme heat events with sleep and cardiovascular health: a scoping review. Syst Rev 2025;14(1):19.ArticlePubMedPMCPDF
- 38. National Institute for Occupational Safety and Health. NIOSH criteria for a recommended standard: occupational exposure to heat and hot environments. NIOSH criteria for a recommended standard: occupational exposure to heat and hot environments. https://books.google.com/books?hl=en&lr=&id=KxD6HGC86S8C&oi=fnd&pg=PR3&dq=Criteria+for+a+Recommended+Standard:+Occupational+Exposure+to+Heat+and+Hot+Environments&ots=-5ZG8jrbHw&sig=o9D5_6eUZzuBpksn5Tl8_RDUUPg. Updated 2018. Accessed September 8, 2025.
- 39. Threshold Limit Value for Chemical Substances and Physical Agents and Biological Exposure Indices. Cincinnati, OH: American Conference of Governmental Industrial Hygienists; 2024.
- 40. Sharma A. The Factory Act, 1948 and social security: concept of factory, manufacturing process, worker and occupier. Indian J Law Leg Res 2023;5(2):1.
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteImpacts of heat on sleep quality among heat-exposed workers: a systematic review
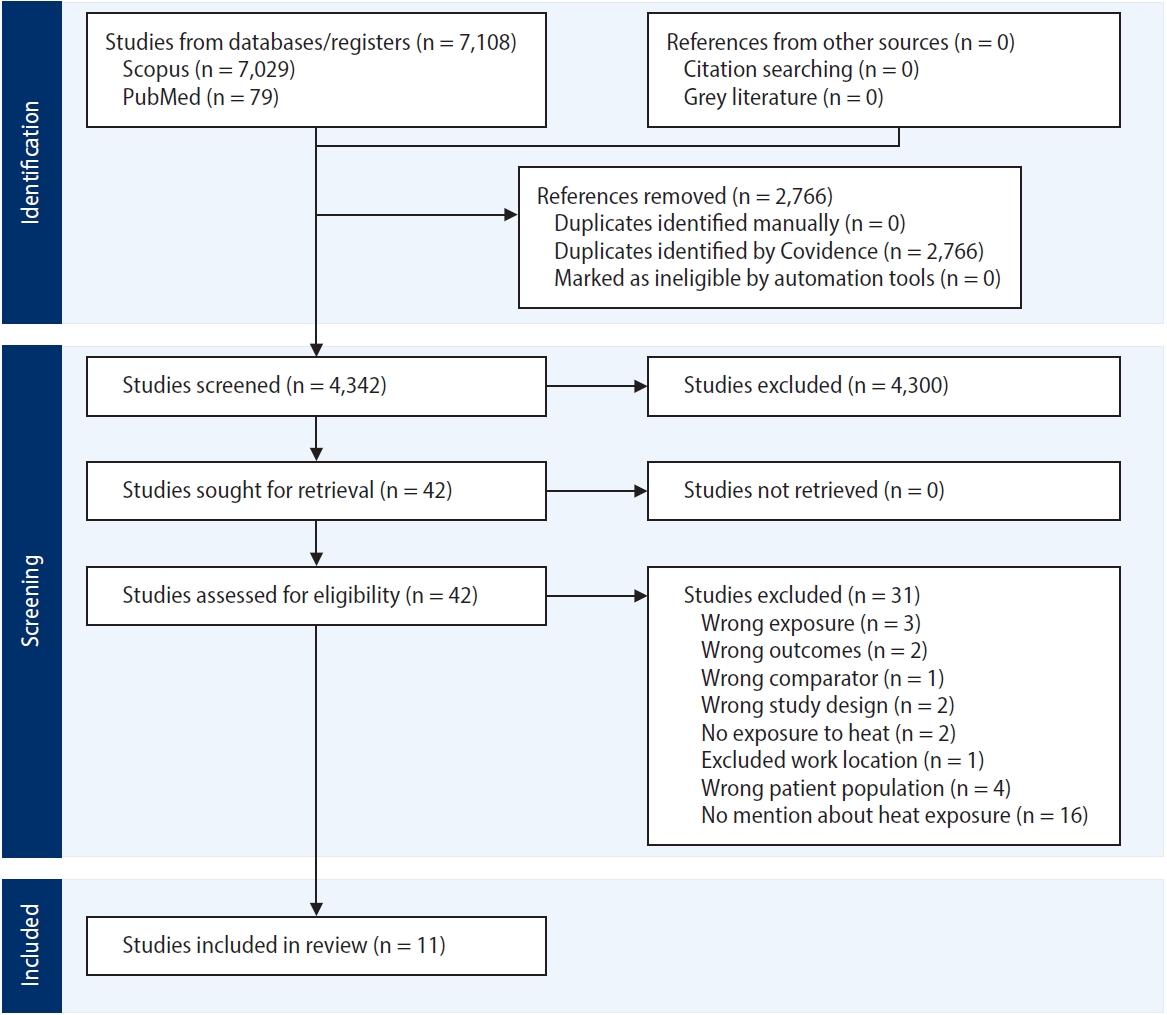
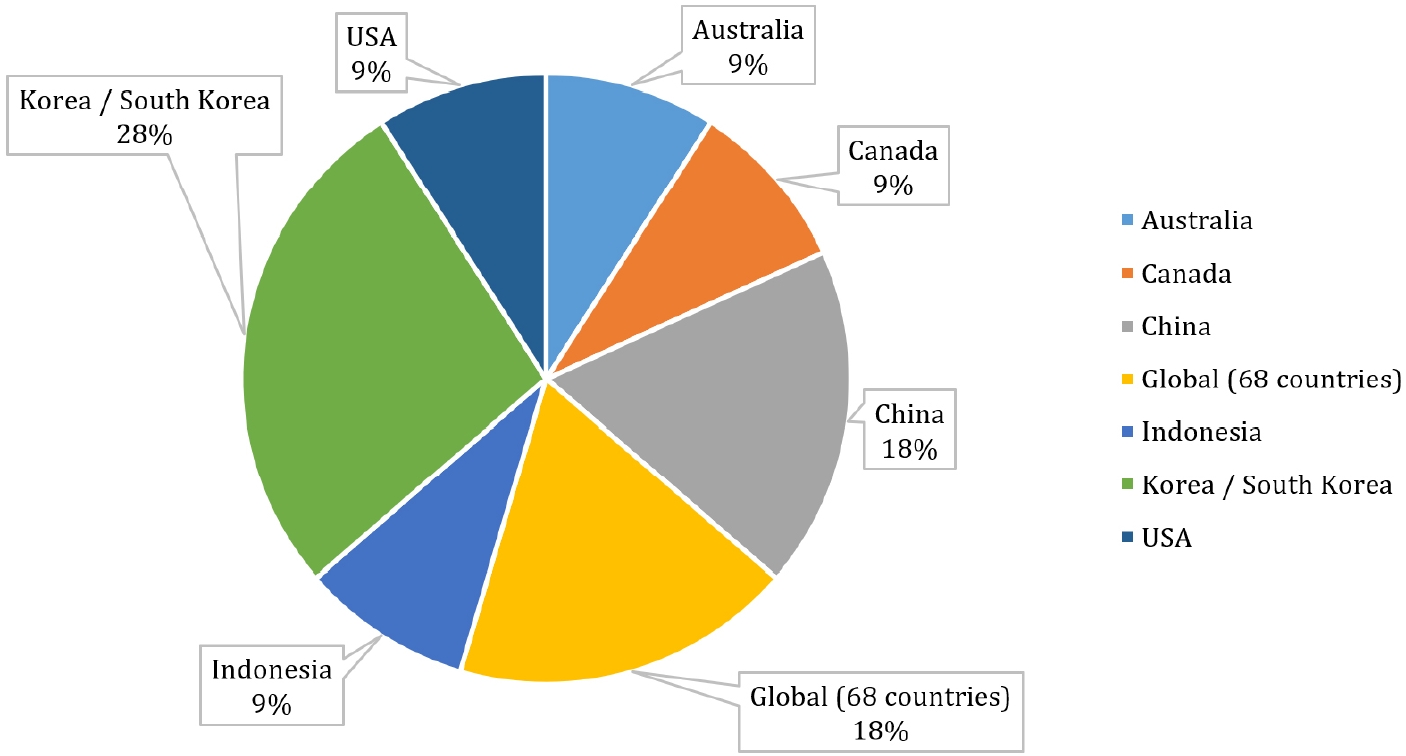
Fig. 1. Covidence screening flow chart (Source: PRISMA guidelines 2022).
Fig. 2. Geographic distribution of included studies.
Fig. 1.
Fig. 2.
Impacts of heat on sleep quality among heat-exposed workers: a systematic review
| Study | Country | Study design | Sample size | Population (occupation/setting) | Exposure measure (WBGT, temperature) | Sleep measure (PSQI, actigraphy, diary) | Key finding | Effect estimate (OR/RR/β/MD) |
|---|---|---|---|---|---|---|---|---|
| Wu et al. (2024)23 | China | Cross-sectional | 952 | Petrochemical workers (enterprise) | WBGT | PSQI, total score; cutoff = 7 used to classify “sleep disorders” | 41.9% Prevalence; risk higher with >40 hour/week, heat, stress | No OR/RR/β/MD reported |
| Minor et al. (2022)27 | Global (68 countries) | Observational (wearable + climate data) | 7M+ sleep records | Workers and general population (68 countries) | Ambient temperature | Actigraphy (wearable fitness bands), total night-time sleep (minutes); sleep onset/offset; and short-sleep binary indicators using standard thresholds <7 hours, <6 hours, <5 hours | Night-time temp >25°C reduces sleep, increases insufficient sleep risk | MD: 1°C rise → ~5–10 minutes loss of sleep (varies by age/sex) |
| Hyun (2024)28 | Korea | National cross-sectional survey | 2,822 | General workforce (nationwide) | Not mentioned about exposure measurement | PSQI (Korean version); cut-off = 8.5 or more denotes presence of sleep disturbance | 49.9% Prevalence; risk higher with two-shift work, >53 hour/week, cold/heat symptoms | Paper reports associations between CHPI domains and sleep |
| Cheong and Gaynanova (2024)25 | USA | Observational (wearable sensing, mixed models) | 30 | Low-income, predominantly Black adults, Houston | Ambient temperature | Actigraphy (GENEActiv: sleep efficiency, TST) | 1°C Rise → ~2% decrease in sleep efficiency; AC mitigated effects | β = −2% sleep efficiency per 1°C increase (AC reduces effect) |
| Legault et al. (2017)26 | Canada | Field study, longitudinal (28–30 days) | 19 | Male underground miners, rotating shifts | Ambient conditions + WBGT (temp, humidity) | Actigraphy (TST, SE, WASO) + PSQI + sleep logs | Poor sleep vs. norms; 61% poor sleepers; degraded attention during night shifts under heat stress | No OR/RR/β/MD reported |
| Park et al. (2022)29 | Korea | Cross-sectional survey (KWCS) | 29,213 | Paid Korean workers (varied industries) | WBGT | Self-report (difficulty falling/maintaining sleep, fatigue) | Severe high-temperature exposure and sleep disturbance (OR: 3.09 in men; 3.30 in women); dose-response effect | OR (severe high temperature): men = 3.09 (95% CI: 2.69–3.56); women = 3.30 (95% CI: 2.81–3.87) |
| Magee et al. (2019)20 | Australia | Cross-sectional survey + Latent Class Analysis (LCA) | 542 employees (aged 18–60) | Australian employees, various sectors | Didn’t mention heat exposure measurement | Bed/wake times, sleep duration (work vs. non-work days), perceived sleep quality | Regular exposure to environmental stressors was linked to insufficient sleep (OR: 3.15) and “owls” (late sleepers; OR: 3.47) | ORs: Regular exposure class associated with insufficient sleep (OR: 3.15; 95% CI: 1.29–7.66) and with owls (OR: 3.47; 95% CI: 1.24–9.71) |
| Rasyid (2023)21 | Indonesia | Cross-sectional | 31 | Rolling mill steel industry workers | Work climate (WBGT) | PSQI, total score; cut off <5 = good sleep; ≥5 = poor sleep (they state PSQI <5 good, >5 poor) | Physical workload (p = 0.031), poor sleep quality (p = 0.047), hot climate (p = 0.002), and high noise (p = 0.009) were significantly associated with work fatigue | No OR/RR/β reported; associations only by p-values: physical workload vs. fatigue (p = 0.031) and sleep quality vs. fatigue (p = 0.047) |
| Minor et al. (2020)12 | 68 Countries worldwide | Observational, panel data analysis | 47,628 Adults, ~7 million nightly sleep records | Workers and general population (accelerometer users) | Night-time outdoor temperature (weather station data) | Wrist-worn accelerometers (sleep duration, onset, offset). Insufficient sleep <7 hours. Heat-associated deviations analyzed in minutes | Hotter nights shortened sleep, especially in older adults and women | Effect estimates (β/MD/percentage-point): Very warm nights (>30°C) reduced sleep by ~14.1 minutes (CI: −17.6 to −10.6). Nights >25°C increased the probability of sleeping <7 hours by ~3.5 percentage points compared with baseline 5–10°C nights |
| Park et al. (2017)30 | South Korea | Case-series using compensation records | 47 Compensated cases (2010–2014) | Heat-exposed workers (construction, cleaning, agroforestry) | WBGT (estimated from meteorological data), heat wave, tropical night | Lack of sleep provided by tropical nights | 95.7% Cases occurred when WBGT exceeded threshold; 61.7% during heat waves | No OR/RR; 95.7% of heat-related cases occurred above WBGT threshold; 61% during heat waves |
| Zhang et al. (2024)24 | China | Cross-sectional survey with ML/DL modelling | 2,393 Valid participants | Petrochemical workers, Fujian Province | Self-reported “temperature discomfort” using a 6-item scale assessing how high temperatures affected work efficiency | Sleep quality and sleep onset difficulty (questionnaire) | 18.0% reported poor sleep; poor sleep linked with higher productivity loss | High temperature exposure (OR: 1.77; 95% CI: 1.12–2.81), weekly >40 hours (OR: 1.74; 95% CI: 1.09–2.82), occupational stress (OR: 2.67; 95% CI: 1.89–3.80) |
| Occupation group | Environmental exposure | Sleep outcomes | Common complaints | Key finding |
|---|---|---|---|---|
| Steel workers | WBGT 28–32°C, radiant heat | Poor PSQI scores | Night sweats, fatigue | Noise + heat interaction worsened outcomes |
| Petrochemical workers | Chronic WBGT exposure (indoor and outdoor tasks) | Higher PSQI (poorer quality) | Restlessness, insomnia, fatigue | Fatigue mediated by long heat exposure |
| Factory workers | Ambient temperature | Higher PSQI scores | Non-restorative sleep | Heat effects compounded by shift timing, similar to low-income workers in poorly ventilated housing |
| Labourers (manual/trades, including outdoor) | WBGT | Higher odds of insufficient sleep and “Owls” | Poor perceived sleep quality | OR: 6.40 (95% CI: 2.45–16.68); night heat reduced TST by ~7–15 minutes |
| General shift workers | WBGT | ~50% Prevalence of disturbed sleep | Poor recovery, insomnia | Survey evidence: vulnerable groups showed stronger effects (elderly, women, low-income) |
| Study | Setting | Environmental measure | Duration/Intensity | Sleep outcomes (PSQI, TST, SE) | Main findings |
|---|---|---|---|---|---|
| Cheong and Gaynanova (2024)25 | Urban, Houston, low-income housing | Person-specific ambient temperature; AC use; outdoor temperature (25–38°C) | 14 Days of continuous monitoring | Sleep efficiency ↓ 2% per °C rise | Vulnerable urban residents (low AC use, poor housing) had worse sleep |
| Park et al. (2022)29 | National (urban and rural) | Self-report workplace temperature (high/low) | Chronic workplace exposures | Sleep disturbance (self-report) | High-temp workplaces (often industrial/urban) had a stronger association with poor sleep |
| Wu et al. (2024)23 | Petrochemical enterprise (Hainan, China) | WBGT, workplace monitoring | Chronic high temp (≥25°C WBGT) | PSQI | Rural-born vs. urban-born workers |
| Park et al. (2017)30 | Korean heat-exposed workers (construction, cleaning, agroforestry) | WBGT, tropical night (>25°C), heat wave (≥33°C for 2+ days) | Acute heat illness episodes (2010–2014) | Lack of sleep inferred from tropical nights | 78.7% of heat-illness cases followed tropical nights, suggesting urban night heat worsens sleep and heat risk |
| Symptom/Complaint | No. of studies reporting | % of total (n = 11) |
|---|---|---|
| Difficulty falling asleep | 7 | 64 |
| Night sweats | 4 | 36 |
| Restlessness | 6 | 54 |
| Non-restorative sleep | 6 | 54 |
| Reduced total sleep time | 5 | 45 |
Table 1. Overview of included studies
WBGT: wet bulb globe temperature; PSQI: Pittsburgh Sleep Quality Index; OR: odds ratio; RR: risk ratio; MD: mean difference; CHPI: Composite Heat Exposure Index; TST: total sleep time; AC: air conditioner; SE: sleep efficiency; WASO: wake after sleep onset; KWCS: Korean Working Conditions Survey; CI: confidence interval; ML: machine learning; DL: deep learning.
Table 2. Summary of the sleep performance among different occupational settings
WBGT: wet bulb globe temperature; PSQI: Pittsburgh Sleep Quality Index; OR: odds ratio; CI: confidence interval; TST: total sleep time.
Table 3. Sleep quality among urban and rural workers
PSQI: Pittsburgh Sleep Quality Index; TST: total sleep time; SE: sleep efficiency; AC: air conditioner; WBGT: wet bulb globe temperature.
Table 4. Reported symptoms/complaints

